You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Healing VisualisationDocument180 pagesHealing Visualisationsol suna100% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- RHU Blue Book 6 - 070852 1Document14 pagesRHU Blue Book 6 - 070852 1Jm Jm100% (1)
- High - Risk Labor and Delivery 2Document106 pagesHigh - Risk Labor and Delivery 2Charmaine Louie Macalanda Lopez-Soriano100% (2)
- TestBank c1Document7 pagesTestBank c1rehab ebraheemNo ratings yet
- Unit 2 Poisons and PoisoningDocument16 pagesUnit 2 Poisons and PoisoningKhar Mel GoNo ratings yet
- Facts and Myths of AgingDocument50 pagesFacts and Myths of AgingangayarkanniNo ratings yet
- MSDS KleratDocument4 pagesMSDS KleratSadhana Sentosa100% (2)
- Nurs 3020 - Erin Final EvaluationDocument14 pagesNurs 3020 - Erin Final Evaluationapi-505854426No ratings yet
- History of medicine from ancient Egypt to IndiaDocument12 pagesHistory of medicine from ancient Egypt to Indiaaditya_2kNo ratings yet
- OceanofPDF - Com Undoctored - Adam KayDocument209 pagesOceanofPDF - Com Undoctored - Adam Kaykatherine grey100% (1)
- Advt No.8/2017: Walk in Interview For Appointment of Engineer Computers / ItDocument2 pagesAdvt No.8/2017: Walk in Interview For Appointment of Engineer Computers / Itbkvuvce8170No ratings yet
- Social and Educational Survey Dashboard KannadaDocument1 pageSocial and Educational Survey Dashboard Kannadabkvuvce8170No ratings yet
- Advt No.8/2017: Walk in Interview For Appointment of Engineer Computers / ItDocument2 pagesAdvt No.8/2017: Walk in Interview For Appointment of Engineer Computers / Itbkvuvce8170No ratings yet
- RS Software BMDocument1 pageRS Software BMbkvuvce8170No ratings yet
- India: Welcome To RedditDocument19 pagesIndia: Welcome To Redditbkvuvce8170No ratings yet
- CS exam questions on computer components, algorithms, C programming, data structures, DBMS, OS and networksDocument4 pagesCS exam questions on computer components, algorithms, C programming, data structures, DBMS, OS and networksbkvuvce8170No ratings yet
- 2012 CVIU IrisReconstruction Galbally PublishedDocument15 pages2012 CVIU IrisReconstruction Galbally Publishedbkvuvce8170No ratings yet
- 2012 CIARP IrisGen PublishedDocument9 pages2012 CIARP IrisGen Publishedbkvuvce8170No ratings yet
- Bangalore Bus Route SearchDocument6 pagesBangalore Bus Route Searchbkvuvce8170No ratings yet
- BMTC 298 Bus Route Timings Bangalore 298A 298B 298C 298D 298E 298F 298G 298H 298L 298J 298K 298M 298MA 298MB 298N 298P 298PADocument7 pagesBMTC 298 Bus Route Timings Bangalore 298A 298B 298C 298D 298E 298F 298G 298H 298L 298J 298K 298M 298MA 298MB 298N 298P 298PAbkvuvce8170No ratings yet
- Reservoir Level Information (Feet) Capacity in TMC Flow DetailsDocument1 pageReservoir Level Information (Feet) Capacity in TMC Flow DetailsNEHA KOTECHANo ratings yet
- Chidambaram WP Cbi Ed21aug19wp30075 78Document1 pageChidambaram WP Cbi Ed21aug19wp30075 78bkvuvce8170No ratings yet
- Consequences of GST Non-Compliance - Offenses and PenaltiesDocument6 pagesConsequences of GST Non-Compliance - Offenses and Penaltiesbkvuvce8170No ratings yet
- Parvati Sweetners - R - 21102013Document3 pagesParvati Sweetners - R - 21102013bkvuvce8170No ratings yet
- Engg Cutoff GenDocument33 pagesEngg Cutoff GenkrishnagdeshpandeNo ratings yet
- Vlsi Website NptelDocument1 pageVlsi Website Nptelbkvuvce8170No ratings yet
- PGCET19 Seat MatrixDocument58 pagesPGCET19 Seat Matrixbkvuvce8170No ratings yet
- Cucumbers: What's New and Beneficial About CucumbersDocument25 pagesCucumbers: What's New and Beneficial About Cucumbersbkvuvce8170No ratings yet
- Aicte TravelDocument5 pagesAicte TravelDeepakNo ratings yet
- RS Software BMDocument1 pageRS Software BMbkvuvce8170No ratings yet
- VTU MTech RegulationsDocument18 pagesVTU MTech RegulationsanjanbsNo ratings yet
- Junior Urban Planners for Smart City ProjectsDocument1 pageJunior Urban Planners for Smart City Projectsbkvuvce8170No ratings yet
- EE Answerkeys Pro2019 PDFDocument4 pagesEE Answerkeys Pro2019 PDFbkvuvce8170No ratings yet
- ELC or IGCDocument3 pagesELC or IGCbkvuvce8170No ratings yet
- BU Ac Members 4MLAs 3Document1 pageBU Ac Members 4MLAs 3bkvuvce8170No ratings yet
- Img 20180404 0001Document1 pageImg 20180404 0001bkvuvce8170No ratings yet
- Img 20180408 0001Document1 pageImg 20180408 0001bkvuvce8170No ratings yet
- Code Course Bachelor's Degree Engineering inDocument19 pagesCode Course Bachelor's Degree Engineering inbkvuvce8170No ratings yet
- Times of India - E-EditionDocument1 pageTimes of India - E-Editionbkvuvce8170No ratings yet
- Mtech - Coll Fee Intake2019Document49 pagesMtech - Coll Fee Intake2019bkvuvce8170No ratings yet
- Apoptosis & Its Relation To CancerDocument16 pagesApoptosis & Its Relation To CancerRohan DuttaNo ratings yet
- Maw Soundbridge ArticleDocument11 pagesMaw Soundbridge ArticleSarah MacNo ratings yet
- CVS Drug TablesDocument12 pagesCVS Drug TablesSaajid AmraNo ratings yet
- Peran Perawat Dalam Manajemen Tim Akses Vaskular HD - Theresia M Toji Pio, RNDocument40 pagesPeran Perawat Dalam Manajemen Tim Akses Vaskular HD - Theresia M Toji Pio, RNjaybeat09No ratings yet
- Bsc2086 Ass. 1 SummerDocument51 pagesBsc2086 Ass. 1 SummerGeico88No ratings yet
- Journal of DiabetesDocument227 pagesJournal of Diabetessupriatin123456No ratings yet
- First Aid Plan ConstructionDocument13 pagesFirst Aid Plan ConstructionUmair KhanNo ratings yet
- 1B Cytokine Instruction Manual-10014905CDocument52 pages1B Cytokine Instruction Manual-10014905CJose EstrellaNo ratings yet
- Genomics in India - Kapil Khandelwal - EquNev CapitalDocument5 pagesGenomics in India - Kapil Khandelwal - EquNev CapitalKapil KhandelwalNo ratings yet
- Sick Role: BY DR P.N. KarimiDocument10 pagesSick Role: BY DR P.N. KarimiGerald Limo Arap ChebiiNo ratings yet
- STROKE-pathophysiology, Diagnosis, and Management, 4th EditionDocument3 pagesSTROKE-pathophysiology, Diagnosis, and Management, 4th EditionNishi RuciNo ratings yet
- Accepted Manuscript: Complementary Therapies in MedicineDocument24 pagesAccepted Manuscript: Complementary Therapies in MedicineAndrea BarresiNo ratings yet
- Body Fluids and CirculationDocument10 pagesBody Fluids and CirculationFree4TechNo ratings yet
- Essay in MapehDocument4 pagesEssay in MapehJane Ikan AlmeroNo ratings yet
- Hesi Hints Part 4Document2 pagesHesi Hints Part 4Sharon TanveerNo ratings yet
- Exploiting DNA Replication Stress For Cancer Treatment: Tajinder Ubhi and Grant W. BrownDocument10 pagesExploiting DNA Replication Stress For Cancer Treatment: Tajinder Ubhi and Grant W. BrownJaganNo ratings yet
- Medical Physics - RespiratoryDocument9 pagesMedical Physics - RespiratoryAhmad wastiNo ratings yet
- ToxicologyDocument9 pagesToxicologyarnav15magicNo ratings yet
- GliclazideDocument5 pagesGliclazideGwyn RosalesNo ratings yet
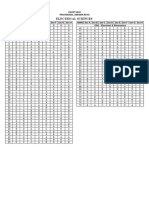
- COMEDK PGET-2008 Answer KeysDocument23 pagesCOMEDK PGET-2008 Answer Keysmobiled2No ratings yet