You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ages and Stages 24 Months QuestionairreDocument8 pagesAges and Stages 24 Months QuestionairreandikaisnaeniNo ratings yet
- List Karyawan Swab Antigen 1 Februari 2021 No Nama Dept JabatanDocument2 pagesList Karyawan Swab Antigen 1 Februari 2021 No Nama Dept JabatanandikaisnaeniNo ratings yet
- Food Safety and Sanitation ChecklistDocument5 pagesFood Safety and Sanitation ChecklistandikaisnaeniNo ratings yet
- Site Walk Finding Report 30 Juni 2020Document4 pagesSite Walk Finding Report 30 Juni 2020andikaisnaeniNo ratings yet
- Site Walk Finding Report 13-Mei-2020Document10 pagesSite Walk Finding Report 13-Mei-2020andikaisnaeniNo ratings yet
- ECG Changes During Septic Shock PDFDocument10 pagesECG Changes During Septic Shock PDFandikaisnaeniNo ratings yet
- Asuhan Keperawatan: Diabetic Ketoacidosis Hyperglycemic Hyperosmolar StateDocument50 pagesAsuhan Keperawatan: Diabetic Ketoacidosis Hyperglycemic Hyperosmolar StateandikaisnaeniNo ratings yet
- Fish Bone Analysis: Irman Somantri, S.Kp. M.KepDocument20 pagesFish Bone Analysis: Irman Somantri, S.Kp. M.KepandikaisnaeniNo ratings yet
- Meta-Analysis of Randomized Controlled Trials of The Efficacy of Propolis Mouthwash in Cancer Therapy-Induced Oral MucositisDocument9 pagesMeta-Analysis of Randomized Controlled Trials of The Efficacy of Propolis Mouthwash in Cancer Therapy-Induced Oral MucositisandikaisnaeniNo ratings yet
- IX Paper 2Document19 pagesIX Paper 2shradhasharma2101No ratings yet
- Core Values Revised 3Document4 pagesCore Values Revised 3api-457909911No ratings yet
- MAELLT Brochure 2006-1Document2 pagesMAELLT Brochure 2006-1Ryan Glenn Cedan CondaNo ratings yet
- Final Research Report - LP and AfDocument147 pagesFinal Research Report - LP and Afapi-636943816No ratings yet
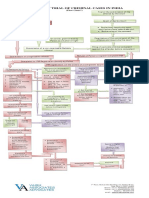
- Process of Trial of Criminal Cases in India (Flow Chart)Document1 pageProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- Design Engineering JourneyDocument159 pagesDesign Engineering JourneyKarenNo ratings yet
- Creative WritingDocument13 pagesCreative WritingBeberly Kim AmaroNo ratings yet
- D245S 734046 Om enDocument90 pagesD245S 734046 Om enEndro Accoustic100% (1)
- Basketball Coaching ToolboxDocument71 pagesBasketball Coaching Toolboxmensrea0No ratings yet
- Grimshaw v. Ford Motor CoDocument35 pagesGrimshaw v. Ford Motor CozichenNo ratings yet
- SDS Jojoba Wax Beads 2860Document7 pagesSDS Jojoba Wax Beads 2860swerNo ratings yet
- PolygonsDocument23 pagesPolygonsPietrelle Liana PuruggananNo ratings yet
- Using Open-Ended Tools in Facilitating Mathematics and Science LearningDocument59 pagesUsing Open-Ended Tools in Facilitating Mathematics and Science LearningDomina Jayne PagapulaanNo ratings yet
- Welcome To UnixDocument14 pagesWelcome To UnixSrinivas KankanampatiNo ratings yet
- 13 Reasons Why Discussion GuideDocument115 pages13 Reasons Why Discussion GuideEC Pisano RiggioNo ratings yet
- Keywords:-Career Levels, Employee Competency, Job: Satisfaction, Organizational CapabilityDocument9 pagesKeywords:-Career Levels, Employee Competency, Job: Satisfaction, Organizational CapabilityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Designation of Mam EdenDocument2 pagesDesignation of Mam EdenNHASSER PASANDALANNo ratings yet
- MMDA v. Viron Transportation CoDocument3 pagesMMDA v. Viron Transportation CoTtlrpqNo ratings yet
- Bus Terminal Building AreasDocument3 pagesBus Terminal Building AreasRohit Kashyap100% (1)
- Articles of IncorporationDocument2 pagesArticles of IncorporationLegal Forms100% (1)
- Personal Details: Your Application Form Has Been Submitted Successfully. Payment Is SuccessfulDocument6 pagesPersonal Details: Your Application Form Has Been Submitted Successfully. Payment Is SuccessfulKanchanNo ratings yet
- Yeb2019 Template MhayDocument9 pagesYeb2019 Template MhayloretaNo ratings yet
- Dolomite in Manila Bay A Big HitDocument3 pagesDolomite in Manila Bay A Big HitJoanaPauline FloresNo ratings yet
- Walsh January Arrest Sherrif Records Pgs 10601-10700Document99 pagesWalsh January Arrest Sherrif Records Pgs 10601-10700columbinefamilyrequest100% (1)
- ARCODE UCM Test Instructions V13.EnDocument4 pagesARCODE UCM Test Instructions V13.EnHenri KleineNo ratings yet
- TEMPLATE Keputusan Peperiksaan THP 1Document49 pagesTEMPLATE Keputusan Peperiksaan THP 1SABERI BIN BANDU KPM-GuruNo ratings yet
- 2019 - List of Equipment, Tools & MaterialsDocument3 pages2019 - List of Equipment, Tools & Materialsreynald manzanoNo ratings yet
- Downloaded From Manuals Search EngineDocument29 pagesDownloaded From Manuals Search EnginehaivermelosantanderNo ratings yet
- Owners Manual Goodman GPC GPHDocument49 pagesOwners Manual Goodman GPC GPHJuan José SanchezNo ratings yet
- 1, Philippine ConstitutionDocument2 pages1, Philippine ConstitutionJasmin KumarNo ratings yet