You might also like
- Assembling Your Antenna SystemDocument27 pagesAssembling Your Antenna SystemKam MusNo ratings yet
- Ahriman's Prophecy Walk ThroughDocument106 pagesAhriman's Prophecy Walk ThroughAngga Nata100% (1)
- Pharmaceutical Industry: A Close LookDocument8 pagesPharmaceutical Industry: A Close LookVikramSubramanianNo ratings yet
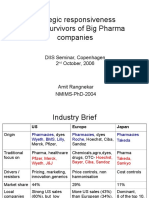
- Global Pharma StrategyDocument15 pagesGlobal Pharma StrategyDr Amit RangnekarNo ratings yet
- Marked Allen - Chap - 1 - Art, Science and Technology of Pharmaceutical Compounding, 4eDocument18 pagesMarked Allen - Chap - 1 - Art, Science and Technology of Pharmaceutical Compounding, 4emamun_ruNo ratings yet
- Promotional Strategies in Pharmaceutical Industry - A Strategic ComprehensionDocument10 pagesPromotional Strategies in Pharmaceutical Industry - A Strategic ComprehensionSmitii SatputeNo ratings yet
- Types of Pharmaceutical Distributors and WholesalersDocument5 pagesTypes of Pharmaceutical Distributors and WholesalersArrowedge LtdNo ratings yet
- OTC Drug Market in India 2011 - Value Chain and Regulation, Competition, Strategic RecommendationsDocument27 pagesOTC Drug Market in India 2011 - Value Chain and Regulation, Competition, Strategic RecommendationsVishnursby100% (1)
- DpcoDocument41 pagesDpcodrugdrugNo ratings yet
- NBPME Part II 2008 Practice Tests 1-3Document49 pagesNBPME Part II 2008 Practice Tests 1-3Vinay Matai50% (2)
- Cognitive InfocommunicationsDocument229 pagesCognitive Infocommunicationsradhakodirekka8732No ratings yet
- Advertising in Pharmaceutical Industry in IndiaDocument9 pagesAdvertising in Pharmaceutical Industry in IndiaMegha SinghNo ratings yet
- Selling Skills PPT LaunchDocument29 pagesSelling Skills PPT LaunchMohamed Ahmed AliNo ratings yet
- Lecture - Three (Pharma Marketing)Document44 pagesLecture - Three (Pharma Marketing)Sajid Ali MaariNo ratings yet
- Rosuvastatinfinal 150826105740 Lva1 App6892 PDFDocument61 pagesRosuvastatinfinal 150826105740 Lva1 App6892 PDFVũ Nguyễn Quỳnh TrangNo ratings yet
- 11-26-2018 Maryland Pharmacy Technician Consensus Conference ReportDocument18 pages11-26-2018 Maryland Pharmacy Technician Consensus Conference ReportSun Jin100% (1)
- CVS HealthDocument4 pagesCVS Healthsalman sheikhNo ratings yet
- Introduction To Cavitation in Pumps and Their TypesDocument12 pagesIntroduction To Cavitation in Pumps and Their TypesMujadid Khawaja100% (1)
- Vitamin D Supplements in The Indian MarketDocument15 pagesVitamin D Supplements in The Indian Marketpartha9sarathi9ainNo ratings yet
- Presentation Marketing and Distribution ChannelsDocument15 pagesPresentation Marketing and Distribution Channelsavtarsingsadaf_28176No ratings yet
- ExportDocument28 pagesExportSunil PatelNo ratings yet
- Fin 320 - Individual AssignmentDocument14 pagesFin 320 - Individual AssignmentAnis Umaira Mohd LutpiNo ratings yet
- Battle Group Builder + Commonwealth Infantry Roster - Wargames DesignDocument12 pagesBattle Group Builder + Commonwealth Infantry Roster - Wargames DesignPete PoliNo ratings yet
- Ranbaxy DistributionDocument19 pagesRanbaxy DistributionNikhil SoniNo ratings yet
- 2015.15009.fundamental Principles of Physical Chemistry - Text PDFDocument782 pages2015.15009.fundamental Principles of Physical Chemistry - Text PDFAnoif Naputo Aidnam100% (1)
- What Is The Requirements and Challenges One Has To Face To Start Pharmaceutical Manufacturing Unit? Pharma Franchise HelpDocument5 pagesWhat Is The Requirements and Challenges One Has To Face To Start Pharmaceutical Manufacturing Unit? Pharma Franchise Helpخبراء التصنيع الدوائي-اليمنNo ratings yet
- Bahrain Exam FeeDocument2 pagesBahrain Exam FeeDr-Jahanzaib GondalNo ratings yet
- Aescul Pharma Company ProfileDocument12 pagesAescul Pharma Company ProfileAlapati PharmaNo ratings yet
- Direct-to-Consumer Pharmaceutical AdvertisingDocument10 pagesDirect-to-Consumer Pharmaceutical AdvertisingNag ArjunNo ratings yet
- Marketing Plan of UrsodexDocument8 pagesMarketing Plan of UrsodexabrarmahirNo ratings yet
- RCPA Prescription Audit Identify Target Customers Assess CustomerDocument14 pagesRCPA Prescription Audit Identify Target Customers Assess Customersubhojitnayek100% (2)
- Minutes of 244th Meeting of Registration BoardDocument268 pagesMinutes of 244th Meeting of Registration BoardSarfarazpk1100% (2)
- Jan Aushadhi Scheme New BusinessplanDocument36 pagesJan Aushadhi Scheme New BusinessplaniddrxNo ratings yet
- Pharmaceutical Market in GeorgiaDocument31 pagesPharmaceutical Market in GeorgiaTIGeorgia100% (1)
- Introduction & Profile Note - InDIAGRODocument7 pagesIntroduction & Profile Note - InDIAGROPooja RathiNo ratings yet
- Results Press Release For December 31, 2016 (Result)Document4 pagesResults Press Release For December 31, 2016 (Result)Shyam SunderNo ratings yet
- Guidelines For Registration of Imported Drug Products in NigeriaDocument7 pagesGuidelines For Registration of Imported Drug Products in NigeriaTueNo ratings yet
- Drug Registration and Essential DrugsDocument42 pagesDrug Registration and Essential DrugsJeyanthakumar RasarathinamNo ratings yet
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocument83 pagesAtherosclerosis, Dyslipidaemia and Diabetes SlidesWee DaliNo ratings yet
- EmblemCorp Presentation August2016Document25 pagesEmblemCorp Presentation August2016NopolarbearsNo ratings yet
- Appendix B - Product Name Sorted by Applicant: December 2019 - Approved Drug Product ListDocument200 pagesAppendix B - Product Name Sorted by Applicant: December 2019 - Approved Drug Product ListlichenresearchNo ratings yet
- Guidelines For Registration of Pharmaceutical Premises in Nigeria by Pharm Saidu BurjiDocument10 pagesGuidelines For Registration of Pharmaceutical Premises in Nigeria by Pharm Saidu BurjiYPS NetworkNo ratings yet
- Ghana Pharmaceutical MarketDocument98 pagesGhana Pharmaceutical MarketnaleesayajNo ratings yet
- Recruitment and Selection Process of Southeast Bank LimitedDocument23 pagesRecruitment and Selection Process of Southeast Bank LimitedRuhul Amin Rahat0% (1)
- The Growth of The Marijuana Industry Warrants Increased Tax Compliance Efforts and Additional GuidanceDocument53 pagesThe Growth of The Marijuana Industry Warrants Increased Tax Compliance Efforts and Additional GuidancesandydocsNo ratings yet
- Pharmaceutical IndustryDocument11 pagesPharmaceutical IndustryAbid Ali KhanNo ratings yet
- Class 1 Indian Medical Council ActDocument40 pagesClass 1 Indian Medical Council ActJanet SweetyNo ratings yet
- Pharmacist StudyDocument100 pagesPharmacist StudyPrajakta ModiNo ratings yet
- Pharmacy How To Establishment in PakistanDocument7 pagesPharmacy How To Establishment in PakistansobiaNo ratings yet
- COPPDocument1 pageCOPPYogesh ChaudhariNo ratings yet
- PharmacyDocument42 pagesPharmacyOpsonin PharmaNo ratings yet
- Ferozsons Daily Sales Stock Statement-07052018Document6 pagesFerozsons Daily Sales Stock Statement-07052018Zain MalikNo ratings yet
- Square PharmaDocument2 pagesSquare PharmaJobaiyer AlamNo ratings yet
- Expanding Access To Emergency Contraceptive Pills: Promoting Pharmacist/Prescriber Collaborative AgreementsDocument57 pagesExpanding Access To Emergency Contraceptive Pills: Promoting Pharmacist/Prescriber Collaborative AgreementsRobert CantemprateNo ratings yet
- Registration PathwayDocument12 pagesRegistration PathwayABC DFGHINo ratings yet
- Difference Between Generic and Brand NameDocument3 pagesDifference Between Generic and Brand NameNoor AliNo ratings yet
- Project On Qarshi Jam e Shirin: University of Central PunjabDocument21 pagesProject On Qarshi Jam e Shirin: University of Central PunjabDanish SalmanNo ratings yet
- Check List For Scrutinization of Registration Application DossiersDocument10 pagesCheck List For Scrutinization of Registration Application DossiersTayyab Tahir100% (1)
- Approved Drug ProductsDocument1,298 pagesApproved Drug ProductsSaharNo ratings yet
- Problems and Prospects of Sales Promotion in Pharmaceutical Marketing CommunicationDocument5 pagesProblems and Prospects of Sales Promotion in Pharmaceutical Marketing CommunicationsarafsaurabhgNo ratings yet
- Compassionate Sciences Inc NorthernAPPDocument72 pagesCompassionate Sciences Inc NorthernAPPNew Jersey marijuana documentsNo ratings yet
- Drug Registration ThailandDocument27 pagesDrug Registration Thailandelpaso25No ratings yet
- The New Trends of Drug R&D Outsourcing in China and IndiaDocument20 pagesThe New Trends of Drug R&D Outsourcing in China and Indiajz9826No ratings yet
- Pharmacoeconomics PDFDocument37 pagesPharmacoeconomics PDFGyana SahooNo ratings yet
- Stabicon LabDocument27 pagesStabicon LabMulayam Singh YadavNo ratings yet
- Intern JanataDocument59 pagesIntern JanataKhairul IslamNo ratings yet
- Graph 1: Temperature,° C of Mixture 1 (Naoh-Hcl) Against Time Taken, (Min)Document8 pagesGraph 1: Temperature,° C of Mixture 1 (Naoh-Hcl) Against Time Taken, (Min)LeeshaaLenee Paramanantha KumarNo ratings yet
- Lecture Notes 1 - Finance - Principles of Finance Lecture Notes 1 - Finance - Principles of FinanceDocument7 pagesLecture Notes 1 - Finance - Principles of Finance Lecture Notes 1 - Finance - Principles of FinanceKim Cristian MaañoNo ratings yet
- Micron Serial NOR Flash Memory: 3V, Multiple I/O, 4KB Sector Erase N25Q256A FeaturesDocument92 pagesMicron Serial NOR Flash Memory: 3V, Multiple I/O, 4KB Sector Erase N25Q256A FeaturesAENo ratings yet
- Proceedings IndexDocument3 pagesProceedings IndexHumberto FerreiraNo ratings yet
- Consider Typical Robots Consider Typical RobotsDocument16 pagesConsider Typical Robots Consider Typical RobotsOthers ATBP.No ratings yet
- Cover PageDocument209 pagesCover PageABHISHREE JAINNo ratings yet
- PESTEL AnalysisDocument2 pagesPESTEL AnalysisSayantan NandyNo ratings yet
- IHRM Midterm ASHUVANI 201903040007Document9 pagesIHRM Midterm ASHUVANI 201903040007ashu vaniNo ratings yet
- Product Data Sheet: Type: P25-34/0DDocument1 pageProduct Data Sheet: Type: P25-34/0DAlejandro RustrianNo ratings yet
- D'Shawn M. Haines: 423 East Fox Trail, Williamstown, NJ 08094 (856) 366-7049Document2 pagesD'Shawn M. Haines: 423 East Fox Trail, Williamstown, NJ 08094 (856) 366-7049dshawnNo ratings yet
- Va797h 15 Q 0019 A00001003Document35 pagesVa797h 15 Q 0019 A00001003Hugo GranadosNo ratings yet
- Marichu Gonzales: Work ExperienceDocument2 pagesMarichu Gonzales: Work ExperienceMich NavorNo ratings yet
- AI LabDocument17 pagesAI LabTripti JainNo ratings yet
- Entrance 2021: Indira Gandhi Rashtriya Uran AkademiDocument2 pagesEntrance 2021: Indira Gandhi Rashtriya Uran Akademird meshramNo ratings yet
- IOTA Observers Manual All PagesDocument382 pagesIOTA Observers Manual All PagesMarcelo MartinsNo ratings yet
- Confirmation 2Document11 pagesConfirmation 2حمزة دراغمةNo ratings yet
- 1353apni KakshaDocument43 pages1353apni KakshaArush GautamNo ratings yet
- Axis Bank - Group 4Document34 pagesAxis Bank - Group 4Deep Ghose DastidarNo ratings yet
- Debit Note and Credit NoteDocument2 pagesDebit Note and Credit Noteabdul haseebNo ratings yet
- Datasheet d801001Document6 pagesDatasheet d801001Hammad HussainNo ratings yet
- Train Collision Avoidance SystemDocument4 pagesTrain Collision Avoidance SystemSaurabh GuptaNo ratings yet