You might also like
- Good Health in the Tropics: Advice to Travellers and SettlersFrom EverandGood Health in the Tropics: Advice to Travellers and SettlersNo ratings yet
- Immunization Verification Form 2018Document2 pagesImmunization Verification Form 2018Jawad JamilNo ratings yet
- Immunization InstructionsDocument2 pagesImmunization InstructionsAli SadeqiNo ratings yet
- (No Cash - Check or Money Order Only) : SECTION 2. To Be Completed by The Appropriate Official at The Medical SchoolDocument6 pages(No Cash - Check or Money Order Only) : SECTION 2. To Be Completed by The Appropriate Official at The Medical SchoolParthNo ratings yet
- Immunization Report PDFDocument2 pagesImmunization Report PDFJag UnathNo ratings yet
- VSLO Immunization Form 22-23Document6 pagesVSLO Immunization Form 22-23Will HNo ratings yet
- Univ of Florida ImmunisationDocument2 pagesUniv of Florida ImmunisationPavan Kumar MangipudiNo ratings yet
- Application Form NewDocument2 pagesApplication Form NewImran AdeelNo ratings yet
- Nursing BSCN Year 1 ERV PackageDocument5 pagesNursing BSCN Year 1 ERV PackageroldinpgNo ratings yet
- Pre-Placement Immunization Form (June 2017) BrockDocument2 pagesPre-Placement Immunization Form (June 2017) BrockroldinpgNo ratings yet
- Attachment E-Health Examination ReportDocument6 pagesAttachment E-Health Examination ReportAnonymous RRkuUNNo ratings yet
- Mcu Form International StudentDocument12 pagesMcu Form International StudentJason WongNo ratings yet
- MN - Claim - formVIP PETDocument2 pagesMN - Claim - formVIP PETSusan MurphyNo ratings yet
- Form B - Other Jobs - High - V High Risk TBDocument8 pagesForm B - Other Jobs - High - V High Risk TBMorshed HumayunNo ratings yet
- Instructions: Netherlandsworldwide - NL Coronacheck - Nl/en/printDocument1 pageInstructions: Netherlandsworldwide - NL Coronacheck - Nl/en/printharish402No ratings yet
- ImmunizationCertificate PDFDocument2 pagesImmunizationCertificate PDFAnonymous kq5iEDxxhrNo ratings yet
- PSW Clinical Requirements Package Fall 2023 InternationalDocument16 pagesPSW Clinical Requirements Package Fall 2023 InternationalAnish KumarNo ratings yet
- Non English Immunization RequirementDocument1 pageNon English Immunization RequirementARVIND MNo ratings yet
- 2024 VPD FormFINAL 16012024Document5 pages2024 VPD FormFINAL 16012024dkid9876No ratings yet
- Immunization Form For Students 2019-20 FINAL 2Document2 pagesImmunization Form For Students 2019-20 FINAL 2Rex ChanNo ratings yet
- Pass QRDocument1 pagePass QRАлинка РомановнаNo ratings yet
- 2022 05 02 08-48-58 AmDocument1 page2022 05 02 08-48-58 AmSakib Md. AsifNo ratings yet
- 2021 10 05 05-54-23 AmDocument1 page2021 10 05 05-54-23 AmmizanNo ratings yet
- officialNIA GENTRY2Document1 pageofficialNIA GENTRY2hot134No ratings yet
- 9.2.2021 Public Health AdvisoryDocument2 pages9.2.2021 Public Health AdvisoryJulie RiddleNo ratings yet
- Immunization Record: Form Is Due at OrientationDocument3 pagesImmunization Record: Form Is Due at OrientationCasey JonesNo ratings yet
- Rutgers Immunization FormDocument3 pagesRutgers Immunization Formruhayl khanNo ratings yet
- Anthony Niogan - Health Care Delivery System (104 RLE)Document7 pagesAnthony Niogan - Health Care Delivery System (104 RLE)niogan anthonyNo ratings yet
- Vaccination Requirements of IFMSA Exchange Progam in Israel-9.15Document2 pagesVaccination Requirements of IFMSA Exchange Progam in Israel-9.15Niko DobrilovicNo ratings yet
- Certificate of Immunization FormDocument1 pageCertificate of Immunization FormShaikahamedNo ratings yet
- EXAMPLE Vaccination Certificat NLDocument1 pageEXAMPLE Vaccination Certificat NLJenske VisNo ratings yet
- 292-Report of Rapid Antigen Test ResultsDocument6 pages292-Report of Rapid Antigen Test ResultsNathan CHOWNo ratings yet
- DownloadDocument1 pageDownloadKvm ShellNo ratings yet
- F 006 Admission Form 2023Document2 pagesF 006 Admission Form 2023EJ “EJ” RoseteNo ratings yet
- DR Case Forms Revised March 2022Document1 pageDR Case Forms Revised March 2022epepNo ratings yet
- CUB - Immunisation FormDocument2 pagesCUB - Immunisation FormArcane BeingNo ratings yet
- HealthHistory 3.26.13 W CoversheetDocument3 pagesHealthHistory 3.26.13 W CoversheetEfua GeeNo ratings yet
- Vaccination Requirement International Students 022019Document2 pagesVaccination Requirement International Students 022019KryzNo ratings yet
- Student Immunization Form 2017-2018Document2 pagesStudent Immunization Form 2017-2018Yashu SharmaNo ratings yet
- Vermont School Immunization Exemption Form2.8Document1 pageVermont School Immunization Exemption Form2.8DonnaNo ratings yet
- Immunization Requirement Form - UpdateDocument2 pagesImmunization Requirement Form - UpdateManojkumar ANo ratings yet
- Become a Lukan MDDocument4 pagesBecome a Lukan MDErica Jazzanne LopezNo ratings yet
- CoronaCheck - InternationalDocument4 pagesCoronaCheck - Internationalmathew holeyNo ratings yet
- I Know That My Redeemer LivethDocument3 pagesI Know That My Redeemer LivethMichelle KwokNo ratings yet
- DM MCH Prospectus January 19 Session FinalDocument33 pagesDM MCH Prospectus January 19 Session FinalGHAPRC RUDRAPURNo ratings yet
- College Application Form For Entrance ExamDocument2 pagesCollege Application Form For Entrance ExamlyannercadaNo ratings yet
- Health Information FormDocument13 pagesHealth Information FormArtero-Cavallaro PabloNo ratings yet
- Instructions For Completion of UA Immunization FormDocument4 pagesInstructions For Completion of UA Immunization FormJ StockmanNo ratings yet
- Immunization FormsDocument6 pagesImmunization FormsNadya IrsalinaNo ratings yet
- OMSC Requests Purchase of Medical EquipmentDocument4 pagesOMSC Requests Purchase of Medical Equipmentvanessa edaniolNo ratings yet
- Batch 2 Main, Bed Clinic - JadeDocument28 pagesBatch 2 Main, Bed Clinic - Jadechuchu lalaNo ratings yet
- Guidelines for Returning-to-Work EmployeesDocument10 pagesGuidelines for Returning-to-Work EmployeesTago DinNo ratings yet
- pgDocument12 pagespgpaunlaknityaNo ratings yet
- Private Midwife Business RequirementsDocument5 pagesPrivate Midwife Business RequirementsJacklyn PacibleNo ratings yet
- PEHR Packet 6Document9 pagesPEHR Packet 6Leonardo Zikri ArmandaNo ratings yet
- UPCAT Application Form GuideDocument2 pagesUPCAT Application Form GuideJM TSR0% (1)
- Non Ust 2019 Aug VerDocument4 pagesNon Ust 2019 Aug VerPatrick Lance BenavidezNo ratings yet
- Examinee's Guide - CSE-PPT - 2022-02 (Pandemic Edition)Document20 pagesExaminee's Guide - CSE-PPT - 2022-02 (Pandemic Edition)ZheinzRanceNo ratings yet
- FIU Immunization Documentation FormDocument2 pagesFIU Immunization Documentation FormMO MONo ratings yet
- 2021 10 12 06-53-20 AmDocument1 page2021 10 12 06-53-20 AmMd. Abu SaeidNo ratings yet
- (Amor Amor - Trombon BajoDocument2 pages(Amor Amor - Trombon Bajofgs1323No ratings yet
- CPEBach - Violino IDocument4 pagesCPEBach - Violino Ifgs1323No ratings yet
- Swee Gaudete LowDocument6 pagesSwee Gaudete Lowfgs1323No ratings yet
- Leclair Violin DuoDocument8 pagesLeclair Violin Duofgs1323100% (1)
- Peruvian InvitationDocument1 pagePeruvian Invitationfgs1323No ratings yet
- Chapter 11B: Survey of Database SystemsDocument17 pagesChapter 11B: Survey of Database SystemsMurtaza MoizNo ratings yet
- Manufacturing Egg Trays from Waste PaperDocument17 pagesManufacturing Egg Trays from Waste Paperravibarora86% (7)
- Saudi Arabia Power StationDocument108 pagesSaudi Arabia Power StationEhab HarbNo ratings yet
- PD 957 AND BP 220 HOUSING DESIGN STANDARDSDocument5 pagesPD 957 AND BP 220 HOUSING DESIGN STANDARDSGeraldine F. CalubNo ratings yet
- NETWORK ANALYSIS Chap.8 TWO PORT NETWORK & NETWORK FUNCTIONS PDFDocument34 pagesNETWORK ANALYSIS Chap.8 TWO PORT NETWORK & NETWORK FUNCTIONS PDFsudarshan poojaryNo ratings yet
- Mechanical Engineer Resume - Digambar BhangeDocument3 pagesMechanical Engineer Resume - Digambar BhangeTOP DHAMAKANo ratings yet
- # 6030 PEN OIL: Grade: Industrial Grade Heavy Duty Penetrating OilDocument3 pages# 6030 PEN OIL: Grade: Industrial Grade Heavy Duty Penetrating OilPrakash KumarNo ratings yet
- KernelDocument326 pagesKernelSkyezine Via Kit FoxNo ratings yet
- GestioIP 3.0 Installation GuideDocument17 pagesGestioIP 3.0 Installation GuidepiterasNo ratings yet
- Detector of FM SignalDocument4 pagesDetector of FM SignalR. JaNNaH100% (1)
- Product Data Sheet: Linear Switch - iSSW - 2 C/O - 20A - 250 V AC - 3 PositionsDocument2 pagesProduct Data Sheet: Linear Switch - iSSW - 2 C/O - 20A - 250 V AC - 3 PositionsMR. TNo ratings yet
- Cheat SheetDocument50 pagesCheat SheetAnubhav ChaturvediNo ratings yet
- Auto Temp II Heat Pump: Programmable Thermostat For Single and Multistage Heat Pump SystemsDocument22 pagesAuto Temp II Heat Pump: Programmable Thermostat For Single and Multistage Heat Pump Systemswideband76No ratings yet
- Dissertation ErsatzteilmanagementDocument7 pagesDissertation ErsatzteilmanagementWriteMyEnglishPaperForMeCanada100% (1)
- DC Motor Direction Control ReportDocument6 pagesDC Motor Direction Control ReportEngr Farhanullah SarkiNo ratings yet
- 38.11 Cum Total Qty of 4 Nos. Culvests 38.11x4 152.43 CumDocument14 pages38.11 Cum Total Qty of 4 Nos. Culvests 38.11x4 152.43 CumMandeep SinghNo ratings yet
- Sean Dickerson ResumeDocument3 pagesSean Dickerson ResumeSeanNo ratings yet
- 12 Fa02Document4 pages12 Fa02corsovaNo ratings yet
- Sheet #6Document2 pagesSheet #6AHMED BAKRNo ratings yet
- Amptec Issue 7Document8 pagesAmptec Issue 7Linda Turner-BoothNo ratings yet
- Active Control of Flow Separation Over An Airfoil Using Synthetic JetsDocument9 pagesActive Control of Flow Separation Over An Airfoil Using Synthetic JetsDrSrujana ReddyNo ratings yet
- Grade 6 Science PuzzleDocument4 pagesGrade 6 Science Puzzlemargie riveraNo ratings yet
- Factors Affecting Purchase Intentions in Generation Z Towards Hipster Cafe in Kelantan LOCKEDDocument70 pagesFactors Affecting Purchase Intentions in Generation Z Towards Hipster Cafe in Kelantan LOCKEDlassan199358No ratings yet
- HTML Project RestaurantDocument8 pagesHTML Project RestaurantSandeep Chowdary0% (1)
- PV Design WorksheetDocument4 pagesPV Design WorksheetLarry Walker II100% (1)
- HoltacDocument8 pagesHoltacdargil66No ratings yet
- Carbon Trading: Delaying Transition Away from Fossil FuelsDocument36 pagesCarbon Trading: Delaying Transition Away from Fossil FuelsFitria AyuNo ratings yet
- Documentation of Xabe - FFmpegDocument11 pagesDocumentation of Xabe - FFmpegTomasz ŻmudaNo ratings yet
- CCTV Camera Hack With Google Dork ListDocument3 pagesCCTV Camera Hack With Google Dork ListsarahdianewhalenNo ratings yet
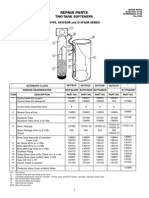
- Star S07FS32DR Water Softener Repair PartsDocument1 pageStar S07FS32DR Water Softener Repair PartsBillNo ratings yet