You might also like
- TENS Electrode Placement PDFDocument34 pagesTENS Electrode Placement PDFjamesmhebertNo ratings yet
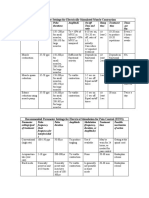
- Parameter Settings for Electrical StimulationDocument3 pagesParameter Settings for Electrical Stimulationpallen100% (5)
- 10 Denmark DVM Earacupuncture WebDocument10 pages10 Denmark DVM Earacupuncture WebDaniel Mendes NettoNo ratings yet
- TENSDocument20 pagesTENSchandran2679100% (2)
- Nspir TAR INC: Inspirstar Product Price ListDocument3 pagesNspir TAR INC: Inspirstar Product Price ListHiten J ThakkerNo ratings yet
- 208 7 20 MicrocurrentDocument2 pages208 7 20 MicrocurrentIon Logofătu Albert50% (2)
- A Skeptical Look at The AcuGraphDocument4 pagesA Skeptical Look at The AcuGraphhjsassoNo ratings yet
- The Crossing Method of Point Selection: by DR Zhou Yu YanDocument3 pagesThe Crossing Method of Point Selection: by DR Zhou Yu YanJose Gregorio ParraNo ratings yet
- Key Concepts in Electrotherapy March 2017Document9 pagesKey Concepts in Electrotherapy March 2017Luis Alvarez Morales100% (1)
- The Effect of Microcurrents On Facial WrinklesDocument9 pagesThe Effect of Microcurrents On Facial WrinklesSofia RivaNo ratings yet
- Frequency Specific Microcurrent Certification ExaminationDocument22 pagesFrequency Specific Microcurrent Certification Examinationdheenadayalan100% (2)
- PEMFUsageGuide v2Document30 pagesPEMFUsageGuide v2JohnNo ratings yet
- The Healing Potency Of Pulsed Electromagnetic Field Therapy: Chronic Pain | Fibromyalgia | Arthritis | Multiple SclerosisFrom EverandThe Healing Potency Of Pulsed Electromagnetic Field Therapy: Chronic Pain | Fibromyalgia | Arthritis | Multiple SclerosisRating: 4 out of 5 stars4/5 (2)
- Peripheral Neuropathy TreatmentDocument3 pagesPeripheral Neuropathy TreatmentSantiago HerreraNo ratings yet
- Ema Sins Trod UtionDocument77 pagesEma Sins Trod Utionfcidral7137100% (1)
- EJOM-9.5.final - A.BruchDocument10 pagesEJOM-9.5.final - A.Bruchmarcia yadavNo ratings yet
- Micro Current CobraDocument3 pagesMicro Current CobraDarren Starwynn100% (1)
- Ryodoraku Research PDFDocument4 pagesRyodoraku Research PDFFaisal MadjidNo ratings yet
- Pain Management by AcupunctureDocument72 pagesPain Management by AcupunctureAna RacovitaNo ratings yet
- PEMF Therapy Guide: A Beginner's 5-Step Quick Start Guide on How to Get Started with PEMF Therapy for Managing Stress, Improving Sleep, and Other Health BenefitsFrom EverandPEMF Therapy Guide: A Beginner's 5-Step Quick Start Guide on How to Get Started with PEMF Therapy for Managing Stress, Improving Sleep, and Other Health BenefitsNo ratings yet
- A Guide To Cold Lasers For Acupuncture and Trigger Point TherapyDocument3 pagesA Guide To Cold Lasers For Acupuncture and Trigger Point TherapyCarl MacCord0% (1)
- Acupuncture On The Cutting Edg@Document10 pagesAcupuncture On The Cutting Edg@Fra LanNo ratings yet
- Basic of EAV PDFDocument17 pagesBasic of EAV PDFmichNo ratings yet
- Harmony Becomes Cacophony When Healthy Cells Become cancerousREV1 1Document6 pagesHarmony Becomes Cacophony When Healthy Cells Become cancerousREV1 1nailsssNo ratings yet
- Carpal Tunnel Syndrome CourseDocument330 pagesCarpal Tunnel Syndrome CourseRyan DeVilleNo ratings yet
- What Is Qi Energy Flow Interpretation of Our Results of Ami Measurements Naohiro Nagayama (Subtle Energies, Vol 21, No 3)Document10 pagesWhat Is Qi Energy Flow Interpretation of Our Results of Ami Measurements Naohiro Nagayama (Subtle Energies, Vol 21, No 3)Cambiador de MundoNo ratings yet
- PEMF Goes Down and What To DO About ItDocument17 pagesPEMF Goes Down and What To DO About Itvibronika100% (3)
- Agnes - Diss VAS NogierDocument114 pagesAgnes - Diss VAS NogierMassiel Socorro Mendez100% (2)
- Transcutaneous Electrical Nerve Stimulation (Tens) and Pain ManagementDocument54 pagesTranscutaneous Electrical Nerve Stimulation (Tens) and Pain ManagementhashfiluthfihNo ratings yet
- Pemf FrequenciesDocument13 pagesPemf FrequenciescumbredinNo ratings yet
- Electroacupuncture According To Voll (EAV)Document1 pageElectroacupuncture According To Voll (EAV)vibe100No ratings yet
- Avazzia Pro-Sport II and BEST RSI Devices ManualDocument131 pagesAvazzia Pro-Sport II and BEST RSI Devices Manualrooiberg100% (3)
- Wound HealingDocument7 pagesWound HealingdivyaNo ratings yet
- The History of Microcurrent Stimulation PDFDocument2 pagesThe History of Microcurrent Stimulation PDFjegm09100% (2)
- The Different Types of Electrotherapy DevicesDocument4 pagesThe Different Types of Electrotherapy DevicescassianohcNo ratings yet
- ECIWO Map MicroAcuDocument2 pagesECIWO Map MicroAcupeter911xNo ratings yet
- Needles and Micro CurrentDocument4 pagesNeedles and Micro CurrentDarren Starwynn100% (2)
- Electro-Acupuncture for Practitioners: Including New Techniques and How Acupuncture and Electro-Acupuncture Really Works ScientificallyFrom EverandElectro-Acupuncture for Practitioners: Including New Techniques and How Acupuncture and Electro-Acupuncture Really Works ScientificallyRating: 5 out of 5 stars5/5 (4)
- MagnetoterapieDocument10 pagesMagnetoterapieHelena PatraNo ratings yet
- Makalah AdabDocument40 pagesMakalah Adabbrain jackNo ratings yet
- EAV Medicine Testing Paper enDocument16 pagesEAV Medicine Testing Paper enGuide WangNo ratings yet
- Laser TherapyDocument7 pagesLaser TherapyGustavo CabanasNo ratings yet
- 59c566785b913 PEMFhowitworksDocument20 pages59c566785b913 PEMFhowitworksWalter SchmittNo ratings yet
- Powerpoint Acupuncture WorksDocument31 pagesPowerpoint Acupuncture WorksrdmhlNo ratings yet
- Su-Jok Acupuncture Methods and Su-Jok Acupuncture Methods and Treatment (Su-Jok Medicine Blog) Treatment (Su-Jok Medicine Blog)Document4 pagesSu-Jok Acupuncture Methods and Su-Jok Acupuncture Methods and Treatment (Su-Jok Medicine Blog) Treatment (Su-Jok Medicine Blog)Dilpreet SinghNo ratings yet
- PEMF Devices Review Meyers PDFDocument5 pagesPEMF Devices Review Meyers PDFdondental100% (2)
- Clinical Trials - Electromagnetic TherapiesDocument7 pagesClinical Trials - Electromagnetic TherapiesClinical-TrialNo ratings yet
- Kyusho Jitsu Alarm Points WorkshopDocument3 pagesKyusho Jitsu Alarm Points Workshopfernando serrano reyesNo ratings yet
- 7.1 Petermann PCLACDocument11 pages7.1 Petermann PCLACbob marley100% (1)
- Laser TheraphyDocument134 pagesLaser Theraphycchlomas4269100% (4)
- Medical Electricity PDFDocument356 pagesMedical Electricity PDFEl INo ratings yet
- Bio-Magnetic Therapy: Healing In Your HandsFrom EverandBio-Magnetic Therapy: Healing In Your HandsNo ratings yet
- (Fu Ke) Acupuncture PointDocument2 pages(Fu Ke) Acupuncture PointWafaa Abdel AzizNo ratings yet
- Filtri 20x20 Per Vino Liquori Birra A Strati FiltrantiDocument9 pagesFiltri 20x20 Per Vino Liquori Birra A Strati FiltrantiRoberto BigliaNo ratings yet
- The Biological Processes Components andDocument19 pagesThe Biological Processes Components andRoberto BigliaNo ratings yet
- A Treatise On The Origin, Nature and Varieties of WineDocument5 pagesA Treatise On The Origin, Nature and Varieties of WineRoberto BigliaNo ratings yet
- Malbec UCDavisDocument4 pagesMalbec UCDavisRoberto BigliaNo ratings yet
- The International Exhibition Co-Operative Wine Society 1914 Bordeaux and BurgundyDocument5 pagesThe International Exhibition Co-Operative Wine Society 1914 Bordeaux and BurgundyRoberto BigliaNo ratings yet
- Aromatherapy For Professionals ENGDocument593 pagesAromatherapy For Professionals ENGcamelia100% (3)
- Malbec TimelineDocument1 pageMalbec TimelineRoberto BigliaNo ratings yet
- How To Build A KegeratorDocument3 pagesHow To Build A KegeratorRoberto BigliaNo ratings yet
- Malbec Eleanore of Aquitaine CahorsDocument7 pagesMalbec Eleanore of Aquitaine CahorsRoberto BigliaNo ratings yet
- Malbec Eleanore of Aquitaine CahorsDocument7 pagesMalbec Eleanore of Aquitaine CahorsRoberto BigliaNo ratings yet
- Acupuncture Modern MedicineDocument400 pagesAcupuncture Modern MedicineRoberto Biglia100% (5)
- Disorders of BloodDocument9 pagesDisorders of BloodRoberto BigliaNo ratings yet
- Ascential Intake Form With InsuranceDocument8 pagesAscential Intake Form With InsuranceRoberto BigliaNo ratings yet
- 77ways ImproveWellbeing PDFDocument257 pages77ways ImproveWellbeing PDFRoberto BigliaNo ratings yet
- Learn To Read Chinese1 UnschuldDocument446 pagesLearn To Read Chinese1 UnschuldRoberto Biglia100% (1)
- Holistic Solutions For Anxiety - Peter Bongiorno PDFDocument290 pagesHolistic Solutions For Anxiety - Peter Bongiorno PDFRoberto Biglia100% (2)
- Inside A FotonDocument306 pagesInside A FotonRoberto Biglia100% (2)
- Energy PhsycologyDocument285 pagesEnergy Phsycologyvanderwalt.paul2286No ratings yet
- Iridology A Complete Guide PDFDocument337 pagesIridology A Complete Guide PDFRoberto Biglia50% (2)
- Thyroid Disorder WMaclean PDFDocument61 pagesThyroid Disorder WMaclean PDFRoberto BigliaNo ratings yet
- Tongue DiagnosisDocument105 pagesTongue DiagnosisJus Summone100% (1)
- Yin Yoga PDFDocument161 pagesYin Yoga PDFRoberto Biglia95% (21)
- Acupuncture Fertility ProtocolDocument1 pageAcupuncture Fertility ProtocolRoberto BigliaNo ratings yet
- Parasitosis TCMDocument277 pagesParasitosis TCMRoberto Biglia100% (2)
- Uhf Leaky Feeder Rev CDocument4 pagesUhf Leaky Feeder Rev CLuis Isaac PadillaNo ratings yet
- Life of A Landfill PumpDocument50 pagesLife of A Landfill PumpumidNo ratings yet
- KINETIC THEORY OF GASES TUTORIALDocument6 pagesKINETIC THEORY OF GASES TUTORIALMat SyafiqNo ratings yet
- 24.postpartum Period-Physiological Changes in The MotherDocument16 pages24.postpartum Period-Physiological Changes in The MotherHem KumariNo ratings yet
- FST Handbook 2014-Final Copy 1 PDFDocument382 pagesFST Handbook 2014-Final Copy 1 PDFDelvon DownerNo ratings yet
- Lightwave Maya 3D TutorialsDocument8 pagesLightwave Maya 3D TutorialsrandfranNo ratings yet
- Sradham ChecklistDocument9 pagesSradham ChecklistpswaminathanNo ratings yet
- ASA 2018 Catalog WebDocument48 pagesASA 2018 Catalog WebglmedinaNo ratings yet
- Elevator Traction Machine CatalogDocument24 pagesElevator Traction Machine CatalogRafif100% (1)
- Design of Fixed Column Base JointsDocument23 pagesDesign of Fixed Column Base JointsLanfranco CorniaNo ratings yet
- AI Model Sentiment AnalysisDocument6 pagesAI Model Sentiment AnalysisNeeraja RanjithNo ratings yet
- Validation Master PlanDocument27 pagesValidation Master PlanPrashansa Shrestha85% (13)
- Hypophosphatemic Rickets: Etiology, Clinical Features and TreatmentDocument6 pagesHypophosphatemic Rickets: Etiology, Clinical Features and TreatmentDeysi Blanco CohuoNo ratings yet
- Motor GraderDocument24 pagesMotor GraderRafael OtuboguatiaNo ratings yet
- IS 4991 (1968) - Criteria For Blast Resistant Design of Structures For Explosions Above Ground-TableDocument1 pageIS 4991 (1968) - Criteria For Blast Resistant Design of Structures For Explosions Above Ground-TableRenieNo ratings yet
- ML AiDocument2 pagesML AiSUYASH SHARTHINo ratings yet
- Brochure Personal CareDocument38 pagesBrochure Personal CarechayanunNo ratings yet
- Pharmacokinetics and Drug EffectsDocument11 pagesPharmacokinetics and Drug Effectsmanilyn dacoNo ratings yet
- SRS Design Guidelines PDFDocument46 pagesSRS Design Guidelines PDFLia FernandaNo ratings yet
- Soil LiquefactionDocument12 pagesSoil LiquefactionKikin Kikin PelukaNo ratings yet
- Man Instructions PDFDocument4 pagesMan Instructions PDFAleksandar NikolovskiNo ratings yet
- CAE The Most Comprehensive and Easy-To-Use Ultrasound SimulatorDocument2 pagesCAE The Most Comprehensive and Easy-To-Use Ultrasound Simulatorjfrías_2No ratings yet
- Revolutionizing Energy Harvesting Harnessing Ambient Solar Energy For Enhanced Electric Power GenerationDocument14 pagesRevolutionizing Energy Harvesting Harnessing Ambient Solar Energy For Enhanced Electric Power GenerationKIU PUBLICATION AND EXTENSIONNo ratings yet
- Answer Key p2 p1Document95 pagesAnswer Key p2 p1Nafisa AliNo ratings yet
- Aortic Stenosis, Mitral Regurgitation, Pulmonary Stenosis, and Tricuspid Regurgitation: Causes, Symptoms, Signs, and TreatmentDocument7 pagesAortic Stenosis, Mitral Regurgitation, Pulmonary Stenosis, and Tricuspid Regurgitation: Causes, Symptoms, Signs, and TreatmentChuu Suen TayNo ratings yet
- Material and Energy Balance: PN Husna Binti ZulkiflyDocument108 pagesMaterial and Energy Balance: PN Husna Binti ZulkiflyFiras 01No ratings yet
- 2019 Course CatalogDocument31 pages2019 Course CatalogDeepen SharmaNo ratings yet
- KoyoDocument4 pagesKoyovichitNo ratings yet
- The Temple of ChaosDocument43 pagesThe Temple of ChaosGauthier GohorryNo ratings yet
- Tetracyclines: Dr. Md. Rageeb Md. Usman Associate Professor Department of PharmacognosyDocument21 pagesTetracyclines: Dr. Md. Rageeb Md. Usman Associate Professor Department of PharmacognosyAnonymous TCbZigVqNo ratings yet