You might also like
- Specification For PVC Door & UPVC - WindowDocument16 pagesSpecification For PVC Door & UPVC - Windowsurbhi aggarwalNo ratings yet
- DH 301 To 500 Bedded Revised DraftDocument162 pagesDH 301 To 500 Bedded Revised Draftdemullu reddiNo ratings yet
- Hospital and Healthcare FacilitiesDocument23 pagesHospital and Healthcare FacilitiesGueanne ConsolacionNo ratings yet
- Crif Door Window Detail-601Document1 pageCrif Door Window Detail-601surbhi aggarwalNo ratings yet
- Curtain Wall PDFDocument257 pagesCurtain Wall PDFsurbhi aggarwalNo ratings yet
- Passive Cooling TechniquesDocument15 pagesPassive Cooling TechniquesmadhurimaroyNo ratings yet
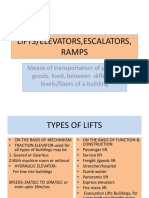
- Lifts & EscalatorsDocument33 pagesLifts & Escalatorssurbhi aggarwal100% (2)
- UHS Adult Major Trauma GuidelinesDocument241 pagesUHS Adult Major Trauma Guidelinesibeardsell1100% (2)
- Classification of HospitalDocument38 pagesClassification of Hospitaljennie jungNo ratings yet
- Non Verbal CommunicationDocument11 pagesNon Verbal Communicationsurbhi aggarwal75% (4)
- Planning and Organizing of HospitalDocument36 pagesPlanning and Organizing of HospitalMamta Poonia100% (1)
- Wartsila TB 2stroke Troubleshooting & Maintenance On Injection Control UnitDocument21 pagesWartsila TB 2stroke Troubleshooting & Maintenance On Injection Control UnitVito Digeo100% (2)
- Planning and Organizing Hospital Units and Ancillary ServicesDocument33 pagesPlanning and Organizing Hospital Units and Ancillary ServicesManisha Thakur100% (1)
- Design A Layout Plan For Speciality Units To Print 2012Document13 pagesDesign A Layout Plan For Speciality Units To Print 2012Anusha Verghese89% (9)
- Oral Hygiene in VentilatorDocument136 pagesOral Hygiene in VentilatorFelicia Risca RyandiniNo ratings yet
- Primary Health CentreDocument22 pagesPrimary Health CentreRakersh Patidar100% (1)
- KSA hospital infection control manualDocument205 pagesKSA hospital infection control manualSalah ElbadawyNo ratings yet
- Organization of HospitalDocument29 pagesOrganization of HospitalAnusha VergheseNo ratings yet
- Hospital Challenges ExplainedDocument26 pagesHospital Challenges Explainedsurbhi aggarwalNo ratings yet
- Hospital Thesis Preparatory GAURAVDocument22 pagesHospital Thesis Preparatory GAURAVGaurav Jain100% (3)
- CurtainDocument257 pagesCurtainvranceanu100% (13)
- Early Warning SystemsDocument7 pagesEarly Warning SystemsJamalNo ratings yet
- A 200 Bed General HospitalDocument74 pagesA 200 Bed General HospitalJiane NavalNo ratings yet
- 200-BED HOSPITAL PROJECT PROFILEDocument40 pages200-BED HOSPITAL PROJECT PROFILEsaleha sultanaNo ratings yet
- Planning & Organizing A Hospital, Unit & Ancillary ServicesDocument31 pagesPlanning & Organizing A Hospital, Unit & Ancillary ServicesSimon Josan100% (4)
- Sabari 200 Beded Hospital Project OfficeDocument40 pagesSabari 200 Beded Hospital Project OfficeGiridhari Prasad NayakNo ratings yet
- What Is Low Cost HousingDocument19 pagesWhat Is Low Cost Housingsurbhi aggarwalNo ratings yet
- Low Cost Housing Design PrinciplesDocument19 pagesLow Cost Housing Design Principlessurbhi aggarwalNo ratings yet
- Hospital Planning PRDocument13 pagesHospital Planning PRSheron DsilvaNo ratings yet
- Essential Factors for Effective Hospital PlanningDocument12 pagesEssential Factors for Effective Hospital PlanningJoe ShewaleNo ratings yet
- Sub District HospitalDocument18 pagesSub District HospitalMd Salman50% (2)
- 500 Bed Thesis ProposalDocument74 pages500 Bed Thesis ProposalJul Parale100% (1)
- Plan & Organiz HospitalDocument119 pagesPlan & Organiz HospitalJobykrishna100% (1)
- Nightingale Institute of Nursing: AssignmentDocument18 pagesNightingale Institute of Nursing: AssignmentDhAiRyA ArOrANo ratings yet
- Data HospitalDocument17 pagesData HospitalSorna VeenaaNo ratings yet
- Acedemic Interaction: Hospital Planning and DesignDocument37 pagesAcedemic Interaction: Hospital Planning and Designyash81rajNo ratings yet
- Indian Public Health StandardsDocument28 pagesIndian Public Health StandardsSneha KumariNo ratings yet
- fokodhariDocument355 pagesfokodhariGLOBOPOINT CONSULTANTSNo ratings yet
- IPHS NormsDocument13 pagesIPHS NormsAnubhav KumarNo ratings yet
- Design Brief - ARC311Document11 pagesDesign Brief - ARC311LagomNo ratings yet
- Mediclaim Polycies Form For EmpanelmentDocument5 pagesMediclaim Polycies Form For EmpanelmentraissgitNo ratings yet
- INTRODUCTIONDocument7 pagesINTRODUCTIONAnusikta PandaNo ratings yet
- AmbulatoryDocument6 pagesAmbulatorysusan_grace123No ratings yet
- DH 201 To 300 Bedded Revised Draft PDFDocument158 pagesDH 201 To 300 Bedded Revised Draft PDFAmit Kumar MishraNo ratings yet
- IPHS Dist Hosp 201 To 300 Bed StandardsDocument158 pagesIPHS Dist Hosp 201 To 300 Bed StandardsHarshit YadavNo ratings yet
- Design of 200 Bed District HospitalDocument4 pagesDesign of 200 Bed District HospitalSudhanshu RanjanNo ratings yet
- Multi-Speciality Hospital Design@Viruthunagar: Data Collection-Background StudyDocument19 pagesMulti-Speciality Hospital Design@Viruthunagar: Data Collection-Background StudygayathiriNo ratings yet
- HOSPITAL NewDocument38 pagesHOSPITAL NewAmala Remigious JNo ratings yet
- IPHS For 31 To 50 Bedded With Comments of Sub Group PDFDocument84 pagesIPHS For 31 To 50 Bedded With Comments of Sub Group PDFsaketNo ratings yet
- Strategic Cost Management and Performance Evaluation: RequiredDocument2 pagesStrategic Cost Management and Performance Evaluation: RequiredAmit GargNo ratings yet
- Major Design Brief ARC070Document7 pagesMajor Design Brief ARC070dolar buhaNo ratings yet
- Updated SDH 31-50 bedded document highlights key changesDocument113 pagesUpdated SDH 31-50 bedded document highlights key changesshanmugapriyasankarNo ratings yet
- Chapter 2 Planning A Hospital BuildingDocument49 pagesChapter 2 Planning A Hospital BuildingSiwani BarmaNo ratings yet
- Final Parameters PDF 2Document11 pagesFinal Parameters PDF 2Nour HamdyNo ratings yet
- Empanel Ment Gud 02062022Document32 pagesEmpanel Ment Gud 02062022Prabhakararao ValluruNo ratings yet
- IPHS For 51 To 100 Bedded With Comments of Sub GroupDocument88 pagesIPHS For 51 To 100 Bedded With Comments of Sub GroupmnagashyamNo ratings yet
- Guidance Note on PIP for ECRP II as on 14.07.2021Document78 pagesGuidance Note on PIP for ECRP II as on 14.07.2021ckakotyNo ratings yet
- Social Planning V-1 0910Document51 pagesSocial Planning V-1 0910mayonheyzNo ratings yet
- Indian Public Health Standards (IPHS) For 31 To 50 Bedded Sub-District/Sub-Divisional HospitalsDocument84 pagesIndian Public Health Standards (IPHS) For 31 To 50 Bedded Sub-District/Sub-Divisional HospitalsFifty OneNo ratings yet
- Updated IPHS Guidelines for 31-50 Bedded Sub-District HospitalsDocument113 pagesUpdated IPHS Guidelines for 31-50 Bedded Sub-District HospitalsLiz Marie GNo ratings yet
- Covid-19 Health-Service-Outline For TouristsDocument92 pagesCovid-19 Health-Service-Outline For TouristsPyae WaNo ratings yet
- Dr. George Trifon HospitalDocument18 pagesDr. George Trifon HospitalIulia NistorNo ratings yet
- Design 8 - Desamparado, Infiesto, MiñozaDocument47 pagesDesign 8 - Desamparado, Infiesto, MiñozaJay-r MiñozaNo ratings yet
- A Case Study On Emerging Services of Trauma Centre of KGMUDocument6 pagesA Case Study On Emerging Services of Trauma Centre of KGMUanashussainNo ratings yet
- Plan - & - Organiz - Hospital IVDocument27 pagesPlan - & - Organiz - Hospital IVmerin sunilNo ratings yet
- D4Document28 pagesD4Ciara AnneNo ratings yet
- Report On 470 Bedded General HospitalDocument16 pagesReport On 470 Bedded General HospitalkuldeepNo ratings yet
- ART20171405Document4 pagesART20171405Rus MiniNo ratings yet
- Lok Nayak Hospital: Aims and Objectives of OrganizationDocument25 pagesLok Nayak Hospital: Aims and Objectives of OrganizationKimsha ConcepcionNo ratings yet
- IPHS For 31 To 50 Bedded With Comments of Sub GroupDocument84 pagesIPHS For 31 To 50 Bedded With Comments of Sub Groupram4uintpt50% (4)
- IPHS SummaryDocument5 pagesIPHS Summaryarch.anupNo ratings yet
- A 500-Bed Suburban General Hospital: Submitted in Partial Fulfillment of The RequirementsDocument74 pagesA 500-Bed Suburban General Hospital: Submitted in Partial Fulfillment of The RequirementsHeindrich Lloyd Mendoza BasiNo ratings yet
- Telemedicine in the ICUFrom EverandTelemedicine in the ICUMatthew A. KoenigNo ratings yet
- Diagnosis of Musculoskeletal Tumors and Tumor-like Conditions: Clinical, Radiological and Histological Correlations - The Rizzoli Case ArchiveFrom EverandDiagnosis of Musculoskeletal Tumors and Tumor-like Conditions: Clinical, Radiological and Histological Correlations - The Rizzoli Case ArchiveNo ratings yet
- Water Installation Section PDFDocument1 pageWater Installation Section PDFsurbhi aggarwalNo ratings yet
- Water Installation Section PDFDocument1 pageWater Installation Section PDFsurbhi aggarwalNo ratings yet
- Stegbar Windows Doors Standard Sizes BrochureDocument19 pagesStegbar Windows Doors Standard Sizes BrochureErika RamosNo ratings yet
- Precast ConcreteDocument18 pagesPrecast Concretesurbhi aggarwalNo ratings yet
- Stegbar Windows Doors Standard Sizes Brochure PDFDocument19 pagesStegbar Windows Doors Standard Sizes Brochure PDFsurbhi aggarwalNo ratings yet
- IPHS guidelines for district hospitalsDocument23 pagesIPHS guidelines for district hospitalssurbhi aggarwalNo ratings yet
- Hospital Def N ManagementDocument14 pagesHospital Def N Managementsurbhi aggarwalNo ratings yet
- Electrical Power Supply & Distribution SystemDocument32 pagesElectrical Power Supply & Distribution Systemsurbhi aggarwalNo ratings yet
- Influential Factors On The Urban Transformation of Cities in Bosnia and Herzegovina in The Period of TransitionDocument11 pagesInfluential Factors On The Urban Transformation of Cities in Bosnia and Herzegovina in The Period of Transitionsurbhi aggarwalNo ratings yet
- University College Accessibility India Design Manual Svayam AICTE Guidelines ModifiedDocument39 pagesUniversity College Accessibility India Design Manual Svayam AICTE Guidelines ModifiedVaishnavi JayakumarNo ratings yet
- AadiDocument16 pagesAadisurbhi aggarwalNo ratings yet
- Barrier Free Enviornment and Design FinalDocument19 pagesBarrier Free Enviornment and Design Finalsurbhi aggarwalNo ratings yet
- 2016 MoUD Harmonised Guidelines On The Norms and Standards For Barrier Free Environment For Persons With Disability and Elderly Persons - DraftDocument135 pages2016 MoUD Harmonised Guidelines On The Norms and Standards For Barrier Free Environment For Persons With Disability and Elderly Persons - DraftVaishnavi Jayakumar100% (2)
- 11 Urban DesignDocument6 pages11 Urban DesignChasity WrightNo ratings yet
- University College Accessibility India Design Manual Svayam AICTE Guidelines ModifiedDocument39 pagesUniversity College Accessibility India Design Manual Svayam AICTE Guidelines ModifiedVaishnavi JayakumarNo ratings yet
- Passive TechniqueDocument29 pagesPassive Techniquesurbhi aggarwalNo ratings yet
- 0 - Hospital Design 2020 PDFDocument3 pages0 - Hospital Design 2020 PDFPriya DharshiniNo ratings yet
- Jessica Foster ResumeDocument3 pagesJessica Foster Resumeapi-292717295No ratings yet
- Mrs. Fakhrya Othman Mohammed EsmailDocument3 pagesMrs. Fakhrya Othman Mohammed EsmailSuhaib Ali ShahNo ratings yet
- NCM18: Care of The Clients With Life Threatening Conditions: Please Answer The Following QuestionsDocument2 pagesNCM18: Care of The Clients With Life Threatening Conditions: Please Answer The Following Questionserjen gamingNo ratings yet
- Nurses: The Unsung Heroes of Patient CareDocument4 pagesNurses: The Unsung Heroes of Patient CareJordan CruzNo ratings yet
- GDocument21 pagesGIvory CollanteNo ratings yet
- Reflective Writing 3Document2 pagesReflective Writing 3Luiza NiyazmetovaNo ratings yet
- Equipment in The Intensive Care Unit - Eng Mohamed AliDocument8 pagesEquipment in The Intensive Care Unit - Eng Mohamed AliMohamed AliNo ratings yet
- Globally Accessible Critical Care SolutionsDocument6 pagesGlobally Accessible Critical Care SolutionsMostafa BadaryNo ratings yet
- A Communication Strategy and Brochure For Relatives of Patients Dying in The ICU - Nejm - Lautrette - 469sa1Document79 pagesA Communication Strategy and Brochure For Relatives of Patients Dying in The ICU - Nejm - Lautrette - 469sa1Manuel PernetasNo ratings yet
- Acute Care Handbook For Physical Therapists 5Th Edition Full ChapterDocument41 pagesAcute Care Handbook For Physical Therapists 5Th Edition Full Chaptergloria.goodwin463100% (20)
- Erica Anacleto ResumeDocument3 pagesErica Anacleto Resumeapi-282272358No ratings yet
- Up Date List of Equipment ListDocument64 pagesUp Date List of Equipment ListShahidul Islam ChowdhuryNo ratings yet
- Mobile Telemedicine System Provides Advanced Emergency CareDocument19 pagesMobile Telemedicine System Provides Advanced Emergency CareRuchi SoniNo ratings yet
- UCD School of Medicine Undergraduate Prospectus 2022-1Document36 pagesUCD School of Medicine Undergraduate Prospectus 2022-1ARab COMPutersNo ratings yet
- Critical Care Handbook for Non-AnaesthetistsDocument23 pagesCritical Care Handbook for Non-AnaesthetistsAtikaNo ratings yet
- Abdominal Compartment Syndrome: By: Adel Ghuloom, MD Lubna Kamaldien, MDDocument42 pagesAbdominal Compartment Syndrome: By: Adel Ghuloom, MD Lubna Kamaldien, MDnanang anacardia Subagyo100% (1)
- Hhac 2018Document13 pagesHhac 2018Mohammad AnasNo ratings yet
- CLJ 2015 8 676 BC07323Document38 pagesCLJ 2015 8 676 BC07323emerituspensieroNo ratings yet
- Jiafm 33 4Document96 pagesJiafm 33 4Sawan PatelNo ratings yet
- Intravenous Maintenance Fluid Therapy in The Pedia PDFDocument18 pagesIntravenous Maintenance Fluid Therapy in The Pedia PDFAdrianRuizNo ratings yet
- The Impact of Paediatric Early Warning Systems: Acute IllnessDocument5 pagesThe Impact of Paediatric Early Warning Systems: Acute IllnessUmi Marfungatun MudrikahNo ratings yet
- KPIs Jan 21, 2019Document113 pagesKPIs Jan 21, 2019JamalNo ratings yet
- LB021 3880 Brochure Rev A5Document5 pagesLB021 3880 Brochure Rev A5juanja83No ratings yet
- Mass Gathering Medecine Hajj PilgrimageDocument10 pagesMass Gathering Medecine Hajj PilgrimageAmira Moch ZakiNo ratings yet