You might also like
- Preparing For An Indian Road Trip - Team-BHPDocument3 pagesPreparing For An Indian Road Trip - Team-BHPwaqar_rohilaNo ratings yet
- HealthMatic Business Solutions Pvt. LTDDocument5 pagesHealthMatic Business Solutions Pvt. LTDwaqar_rohilaNo ratings yet
- 502W045GB Horticulture 5 PreviewDocument4 pages502W045GB Horticulture 5 Previewwaqar_rohilaNo ratings yet
- 10 M Air Rifle Range DimensionsDocument1 page10 M Air Rifle Range Dimensionswaqar_rohilaNo ratings yet
- Lesson 5 Aiming FiringDocument5 pagesLesson 5 Aiming Firingwaqar_rohilaNo ratings yet
- International Pistol Target SelectionDocument4 pagesInternational Pistol Target Selectionwaqar_rohilaNo ratings yet
- Airgun Safetyguide 1Document5 pagesAirgun Safetyguide 1waqar_rohilaNo ratings yet
- 4 HAirRifleProjectBook 2-12-13Document17 pages4 HAirRifleProjectBook 2-12-13waqar_rohilaNo ratings yet
- Airgun Safetyguide-1 PDFDocument16 pagesAirgun Safetyguide-1 PDFwaqar_rohilaNo ratings yet
- AFF (Automated Field Fire) Surface Danger ZoneDocument2 pagesAFF (Automated Field Fire) Surface Danger Zonewaqar_rohilaNo ratings yet
- Target Shooting Equipment IntroductionDocument7 pagesTarget Shooting Equipment Introductionwaqar_rohilaNo ratings yet
- Pistool TrainingDocument16 pagesPistool Trainingwaqar_rohilaNo ratings yet
- Lesson 4 StandingDocument6 pagesLesson 4 Standingwaqar_rohilaNo ratings yet
- Erratta Sheet To Unit 7 11 Jan 05Document5 pagesErratta Sheet To Unit 7 11 Jan 05waqar_rohilaNo ratings yet
- Lesson 6 Sight A Dust MentDocument6 pagesLesson 6 Sight A Dust Mentwaqar_rohilaNo ratings yet
- Expert Insights on Holistic Family TreatmentDocument16 pagesExpert Insights on Holistic Family Treatmentwaqar_rohilaNo ratings yet
- Lesson 7 ProneDocument7 pagesLesson 7 Pronewaqar_rohilaNo ratings yet
- Lesson 8 KneelingDocument5 pagesLesson 8 Kneelingwaqar_rohilaNo ratings yet
- AAP Vision Booklet (Hindi) PDFDocument28 pagesAAP Vision Booklet (Hindi) PDFwaqar_rohilaNo ratings yet
- Lesson 9 PracticeDocument9 pagesLesson 9 Practicewaqar_rohilaNo ratings yet
- Lesson 2 SafetyDocument6 pagesLesson 2 Safetywaqar_rohilaNo ratings yet
- Lesson 10 RulesDocument7 pagesLesson 10 Ruleswaqar_rohilaNo ratings yet
- Rifle Marksmanship D: The Kneeling PositionDocument12 pagesRifle Marksmanship D: The Kneeling Positionwaqar_rohilaNo ratings yet
- Doing BusinessDocument282 pagesDoing BusinessAldax KeelNo ratings yet
- Choosing The Best Dog CrateDocument15 pagesChoosing The Best Dog Cratewaqar_rohilaNo ratings yet
- List of Certification Bodies PDFDocument10 pagesList of Certification Bodies PDFwaqar_rohilaNo ratings yet
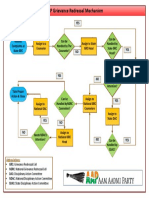
- AAP Grievance Redressal Mechanism: AbbreviationsDocument1 pageAAP Grievance Redressal Mechanism: Abbreviationswaqar_rohilaNo ratings yet
- Agmark Organic Rules-FinalDocument25 pagesAgmark Organic Rules-Finalmapas_salemNo ratings yet
- Artificial Turf FieldDocument2 pagesArtificial Turf Fieldwaqar_rohilaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Total NumbersDocument8 pagesTotal Numbersapi-360930964No ratings yet
- Percutaneous Coronary Interventions For Chronic Total Occlusion 2019Document155 pagesPercutaneous Coronary Interventions For Chronic Total Occlusion 2019mepimplolabotellasNo ratings yet
- Anaphy Concept MappingDocument3 pagesAnaphy Concept MappingArlynn MartinezNo ratings yet
- CB5 C Caridovascular Disease CSHDocument27 pagesCB5 C Caridovascular Disease CSHMarcus WrightNo ratings yet
- Profil Pemberian Nifedipine Kombinasi Metildopa Dan Mgso Pada Pasien Pre-Eklamsi Berat Di Rumah Sakit Daerah Mangusada BadungDocument8 pagesProfil Pemberian Nifedipine Kombinasi Metildopa Dan Mgso Pada Pasien Pre-Eklamsi Berat Di Rumah Sakit Daerah Mangusada BadungPratama InsaniNo ratings yet
- Chapter 17 INTERPRETING ELECROCARDIOGRAMDocument7 pagesChapter 17 INTERPRETING ELECROCARDIOGRAMZahra Margrette SchuckNo ratings yet
- OBAT-OBATAN YANG MEMPENGARUHI SISTEM KARDIOVASKULERDocument51 pagesOBAT-OBATAN YANG MEMPENGARUHI SISTEM KARDIOVASKULERQuswah MaharaniNo ratings yet
- Circulatory System: Heart, Blood Vessels & Their FunctionsDocument17 pagesCirculatory System: Heart, Blood Vessels & Their FunctionskangaanushkaNo ratings yet
- Hands On CPR WorksheetDocument1 pageHands On CPR Worksheetapi-404833978No ratings yet
- Decreased Cardiac OutputDocument2 pagesDecreased Cardiac OutputEdrianne J.100% (2)
- Unit 6 Flash On English Monitoring Vital SignsDocument9 pagesUnit 6 Flash On English Monitoring Vital SignsKartonoNo ratings yet
- Assessment of Victim at The Accident SiteDocument64 pagesAssessment of Victim at The Accident SiteGerald Limo Arap ChebiiNo ratings yet
- Adrenergic Antagonist 2 (Propranolol)Document5 pagesAdrenergic Antagonist 2 (Propranolol)ziad shahinNo ratings yet
- Name: Dheeraj Singh Subject:Urgent Surgery: Critical Care Obstetric Workshop SeriesDocument40 pagesName: Dheeraj Singh Subject:Urgent Surgery: Critical Care Obstetric Workshop SeriesAnkit Tonger AnkyNo ratings yet
- Lifestyle Factors Among Hypertensive - Hypertensive: CopingDocument6 pagesLifestyle Factors Among Hypertensive - Hypertensive: Copingiqra uroojNo ratings yet
- Handwashing TechniqueDocument230 pagesHandwashing Techniquejecyle ludaNo ratings yet
- Kunjungan Agustus 2022Document42 pagesKunjungan Agustus 2022Klinik dr. DarlinaNo ratings yet
- Examination of PlacentaDocument2 pagesExamination of PlacentaAnju MargaretNo ratings yet
- Basic Ecg: A Report By: Clinical Clerk Mary Hazel TeDocument74 pagesBasic Ecg: A Report By: Clinical Clerk Mary Hazel TeHazel Arcosa100% (1)
- Acute MX of StrokeDocument23 pagesAcute MX of StrokeAshish GuragainNo ratings yet
- Jurnal Artikel Feby Nurlia 1907110032Document8 pagesJurnal Artikel Feby Nurlia 1907110032Feby NurLiaNo ratings yet
- Jurnal Internasional Draft 3Document8 pagesJurnal Internasional Draft 3thenytirtaNo ratings yet
- Propranolol Presentation FinalDocument14 pagesPropranolol Presentation FinalVishnu ShindeNo ratings yet
- Abbreviation Meaning: AbdominalDocument3 pagesAbbreviation Meaning: AbdominalMariel GentilesNo ratings yet
- Chest X-Ray InterpretationDocument14 pagesChest X-Ray InterpretationKoya AnushareddyNo ratings yet
- Example 001Document13 pagesExample 001Rishabh SansanwalNo ratings yet
- IschemicheartdiseaseDocument11 pagesIschemicheartdiseaseZaimon MaulionNo ratings yet
- Susanna Price MBBS BSc FRCP EDICM PhD FFICM FESC Consultant Cardiologist & IntensivistDocument4 pagesSusanna Price MBBS BSc FRCP EDICM PhD FFICM FESC Consultant Cardiologist & Intensivistmeenakshi.r.agrawalNo ratings yet
- Hospitalized 67-Year-Old Black Woman MIDocument2 pagesHospitalized 67-Year-Old Black Woman MIMaria Jessica DumdumNo ratings yet
- Acs Guideline PDFDocument56 pagesAcs Guideline PDFPrimasari HijriyahNo ratings yet