You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Population Education of The Philippines: Carlos, Cayla Mae Nepomuceno, Clark Roncal, Meriel BSN 2-CDocument37 pagesPopulation Education of The Philippines: Carlos, Cayla Mae Nepomuceno, Clark Roncal, Meriel BSN 2-CCayla Mae Carlos100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Volleyball: VOLLEYBALL Is A Competitive Sport. Athletes Can Enjoy It Better If They Play With ProfessionalDocument5 pagesVolleyball: VOLLEYBALL Is A Competitive Sport. Athletes Can Enjoy It Better If They Play With ProfessionalCayla Mae CarlosNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Impact of Corporations on the EnvironmentDocument2 pagesThe Impact of Corporations on the EnvironmentCayla Mae CarlosNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Asian Regionalism ReportDocument22 pagesAsian Regionalism ReportCayla Mae Carlos100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- COVIDcasepositiveDocument2 pagesCOVIDcasepositiveKrishna JandhyalaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
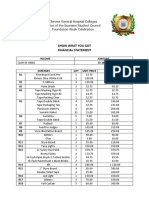
- Show What You GotDocument3 pagesShow What You GotCayla Mae CarlosNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Global EconomyDocument2 pagesThe Global EconomyCayla Mae CarlosNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 1 N-109 MCN 2 LEC Syllabus (2 S, AY 19-20) REVISED PDFDocument7 pages1 N-109 MCN 2 LEC Syllabus (2 S, AY 19-20) REVISED PDFCayla Mae CarlosNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Maternal and Child Nursing QuestionsDocument2 pagesMaternal and Child Nursing QuestionsCayla Mae CarlosNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- PE BasketballDocument12 pagesPE BasketballCayla Mae CarlosNo ratings yet
- Nursing Info Unit I To IIIDocument6 pagesNursing Info Unit I To IIICayla Mae CarlosNo ratings yet
- Bosh (So1) HulmaDocument3 pagesBosh (So1) HulmaCayla Mae CarlosNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Nursing Info Unit I To IIIDocument6 pagesNursing Info Unit I To IIICayla Mae CarlosNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Nursing Info AbstractDocument11 pagesNursing Info AbstractCayla Mae CarlosNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- NifedipineDocument3 pagesNifedipineNovi YulianaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Awarding CeremonyDocument1 pageAwarding CeremonyCayla Mae CarlosNo ratings yet
- Asian Regionalism ReportDocument22 pagesAsian Regionalism ReportCayla Mae Carlos100% (1)
- Chloes AssignmenyDocument4 pagesChloes AssignmenyCayla Mae CarlosNo ratings yet
- Received 1375421425991991Document1 pageReceived 1375421425991991Cayla Mae CarlosNo ratings yet
- TCW Readings GuideDocument4 pagesTCW Readings GuideRose Ann AriolaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Appendix 42 - Instructions - LDDAP-ADADocument2 pagesAppendix 42 - Instructions - LDDAP-ADATesa GD67% (3)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Chinese Hospital College Concepts of GlobalizationDocument1 pageChinese Hospital College Concepts of GlobalizationCayla Mae CarlosNo ratings yet
- Nursing Assessment, Plan, Interventions & Evaluation for Postpartum ConstipationDocument2 pagesNursing Assessment, Plan, Interventions & Evaluation for Postpartum ConstipationCayla Mae CarlosNo ratings yet
- Chinese Hospital College Concepts of GlobalizationDocument1 pageChinese Hospital College Concepts of GlobalizationCayla Mae CarlosNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Appendix 42 - Instructions - LDDAP-ADADocument2 pagesAppendix 42 - Instructions - LDDAP-ADATesa GD67% (3)
- DemoDocument5 pagesDemoCayla Mae CarlosNo ratings yet
- Elpidio QuirinoDocument15 pagesElpidio QuirinoCayla Mae CarlosNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Short Term GoalDocument2 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Short Term GoalCayla Mae CarlosNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Lecture 2-Small Business ManagementDocument108 pagesLecture 2-Small Business ManagementCayla Mae CarlosNo ratings yet
- Mathematicians and their contributionsDocument8 pagesMathematicians and their contributionsCayla Mae CarlosNo ratings yet
- CpE194 Lab Experiment # 1 - MTS-88 FamiliarizationDocument4 pagesCpE194 Lab Experiment # 1 - MTS-88 FamiliarizationLouieMurioNo ratings yet
- Recording and reporting in hospitals and nursing collegesDocument48 pagesRecording and reporting in hospitals and nursing collegesRaja100% (2)
- Literary Text Analysis WorksheetDocument1 pageLiterary Text Analysis Worksheetapi-403444340No ratings yet
- COS1512 202 - 2015 - 1 - BDocument33 pagesCOS1512 202 - 2015 - 1 - BLina Slabbert-van Der Walt100% (1)
- HTTP - WWW - Aphref.aph - Gov.au - House - Committee - Pjcis - nsl2012 - Additional - Discussion Paper PDFDocument61 pagesHTTP - WWW - Aphref.aph - Gov.au - House - Committee - Pjcis - nsl2012 - Additional - Discussion Paper PDFZainul Fikri ZulfikarNo ratings yet
- Growing Up Psychic by Chip Coffey - ExcerptDocument48 pagesGrowing Up Psychic by Chip Coffey - ExcerptCrown Publishing Group100% (1)
- Shailesh Sharma HoroscopeDocument46 pagesShailesh Sharma Horoscopeapi-3818255No ratings yet
- Boston Qualitative Scoring System for Rey-Osterrieth Complex Figure Effective for Detecting Cognitive Impairment in Parkinson's DiseaseDocument9 pagesBoston Qualitative Scoring System for Rey-Osterrieth Complex Figure Effective for Detecting Cognitive Impairment in Parkinson's DiseaseJuanNo ratings yet
- HAU Theology 103 Group Goal Commitment ReportDocument6 pagesHAU Theology 103 Group Goal Commitment ReportEM SagunNo ratings yet
- From Romanticism To NaturalismDocument2 pagesFrom Romanticism To NaturalismBruce ClaryNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Carnot CycleDocument3 pagesCarnot CyclealexontingNo ratings yet
- 07CRMDocument81 pages07CRMsangramlifeNo ratings yet
- S32 Design Studio 3.1: NXP SemiconductorsDocument9 pagesS32 Design Studio 3.1: NXP SemiconductorsThành Chu BáNo ratings yet
- EdiTasc EDocument89 pagesEdiTasc EOglasnik MostarNo ratings yet
- Proportions PosterDocument1 pageProportions Posterapi-214764900No ratings yet
- Policarpio 3 - Refresher GEODocument2 pagesPolicarpio 3 - Refresher GEOJohn RoaNo ratings yet
- Mri 7 TeslaDocument12 pagesMri 7 TeslaJEAN FELLIPE BARROSNo ratings yet
- Laser Plasma Accelerators PDFDocument12 pagesLaser Plasma Accelerators PDFAjit UpadhyayNo ratings yet
- Writing and Presenting A Project Proposal To AcademicsDocument87 pagesWriting and Presenting A Project Proposal To AcademicsAllyNo ratings yet
- Laxmi Thakur (17BIT0384) Anamika Guha (18BIT0483) : Submitted byDocument6 pagesLaxmi Thakur (17BIT0384) Anamika Guha (18BIT0483) : Submitted byLaxmi ThakurNo ratings yet
- Instruction Manual For National Security Threat Map UsersDocument16 pagesInstruction Manual For National Security Threat Map UsersJan KastorNo ratings yet
- Studies On Diffusion Approach of MN Ions Onto Granular Activated CarbonDocument7 pagesStudies On Diffusion Approach of MN Ions Onto Granular Activated CarbonInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Servo Magazine 01 2005Document84 pagesServo Magazine 01 2005dangtq8467% (3)
- Royal DSMDocument16 pagesRoyal DSMSree100% (2)
- Reich Web ADocument34 pagesReich Web Ak1nj3No ratings yet
- Rhythm Music and Education - Dalcroze PDFDocument409 pagesRhythm Music and Education - Dalcroze PDFJhonatas Carmo100% (3)
- 8 DaysDocument337 pages8 Daysprakab100% (1)
- Final Thesis Owura Kofi AmoabengDocument84 pagesFinal Thesis Owura Kofi AmoabengKunal AgarwalNo ratings yet
- McCann MIA CredentialsDocument20 pagesMcCann MIA CredentialsgbertainaNo ratings yet
- JHS SLM 1 Q2 Math Grade 10 32pagesDocument32 pagesJHS SLM 1 Q2 Math Grade 10 32pagesAngel Naiza JimenezNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary of The 48 Laws of Power: by Robert GreeneFrom EverandSummary of The 48 Laws of Power: by Robert GreeneRating: 4.5 out of 5 stars4.5/5 (233)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)