You might also like
- Side-Effects of Topical Steroids: A Long Overdue Revisit: Review ArticleDocument10 pagesSide-Effects of Topical Steroids: A Long Overdue Revisit: Review ArticleVidini Kusuma AjiNo ratings yet
- WF Lab Clin TM RbcsDocument3 pagesWF Lab Clin TM RbcsVidini Kusuma AjiNo ratings yet
- Transfusion of Human Volunteers With Older, Stored Red Blood Cells Produces Extravascular Hemolysis and Circulating Non-Transferrin-Bound IronDocument9 pagesTransfusion of Human Volunteers With Older, Stored Red Blood Cells Produces Extravascular Hemolysis and Circulating Non-Transferrin-Bound IronVidini Kusuma AjiNo ratings yet
- Femur Shaft Fractures in Children: An Epidemiological and Biomechanical StudyDocument71 pagesFemur Shaft Fractures in Children: An Epidemiological and Biomechanical StudyVidini Kusuma AjiNo ratings yet
- The Revised 2014 GINA Strategy Report: Opportunities For ChangeDocument7 pagesThe Revised 2014 GINA Strategy Report: Opportunities For ChangeVidini Kusuma AjiNo ratings yet
- Vaginal DischargeDocument1 pageVaginal DischargeVidini Kusuma AjiNo ratings yet
- Vol.18 No.3 6Document73 pagesVol.18 No.3 6Vidini Kusuma AjiNo ratings yet
- 5 ArticleDocument6 pages5 ArticleVidini Kusuma AjiNo ratings yet
- Safety and Efficacy of Packed Red Blood Cell Transfusions at Different Doses in Very Low Birth Weight InfantsDocument3 pagesSafety and Efficacy of Packed Red Blood Cell Transfusions at Different Doses in Very Low Birth Weight InfantsVidini Kusuma AjiNo ratings yet
- Imaging in Acute Appendicitis: A Review: RK Jain, M Jain, CL Rajak, S Mukherjee, PP Bhattacharyya, MR ShahDocument10 pagesImaging in Acute Appendicitis: A Review: RK Jain, M Jain, CL Rajak, S Mukherjee, PP Bhattacharyya, MR ShahVidini Kusuma AjiNo ratings yet
- Psychosis in Dengue FeverDocument4 pagesPsychosis in Dengue FeverVidini Kusuma AjiNo ratings yet
- Panduan Kesehatan OlahragaDocument1 pagePanduan Kesehatan OlahragaVidini Kusuma AjiNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Textbook of Practical Physiology110718 PDFDocument25 pagesTextbook of Practical Physiology110718 PDFLalit Narayana0% (2)
- BELLADONNADocument2 pagesBELLADONNASuhas IngaleNo ratings yet
- Mechanical Loads - Bone ResponseDocument19 pagesMechanical Loads - Bone ResponselllllAdelalllllNo ratings yet
- Lesson 3.3Document21 pagesLesson 3.3Claude Nathan AlidoNo ratings yet
- Tune Up FitnessDocument6 pagesTune Up FitnessMarsela Giovanni100% (2)
- Respiratory Quiz: Student Academic Learning ServicesDocument4 pagesRespiratory Quiz: Student Academic Learning ServicesFREDRICKNo ratings yet
- AbscessDocument26 pagesAbscessThusith WijayawardenaNo ratings yet
- ZK Article 1954 PDFDocument46 pagesZK Article 1954 PDFJonata ArrudaNo ratings yet
- 11th Bio Botany Book Back 1 Mark Questions With Answer Key English Medium - BakDocument6 pages11th Bio Botany Book Back 1 Mark Questions With Answer Key English Medium - BakShriya RameshNo ratings yet
- Citrate Activates Accoa Carboxylase (Fa Synthesis) and F-1,6 BP (Gluconeogenesis)Document6 pagesCitrate Activates Accoa Carboxylase (Fa Synthesis) and F-1,6 BP (Gluconeogenesis)Nahome YebassewNo ratings yet
- EnalaprilDocument32 pagesEnalaprilYeyenJaejoongNo ratings yet
- 05 HypoxiaDocument75 pages05 HypoxiaShri PravallikaNo ratings yet
- Lambou Delto PectoralDocument9 pagesLambou Delto PectoralalexNo ratings yet
- 1990-Fleming Suturing Method and PainDocument7 pages1990-Fleming Suturing Method and PainAnonymous bq4KY0mcWG0% (1)
- Measuring Heart Rate Variability Using ADocument12 pagesMeasuring Heart Rate Variability Using Adjordjevet1980No ratings yet
- Bio PP1 QS Pre-Mock 2024.Document9 pagesBio PP1 QS Pre-Mock 2024.Elvis KemboiNo ratings yet
- Left To Right ShuntDocument7 pagesLeft To Right Shuntanindhita anestyaNo ratings yet
- TramadolDocument2 pagesTramadolPapaindoNo ratings yet
- Active Principle: Lecture 10 Pharm Sci/Chem 177, University of California, IrvineDocument52 pagesActive Principle: Lecture 10 Pharm Sci/Chem 177, University of California, IrvineVivian PhamNo ratings yet
- 10 11648 J Ajim 20180606 14Document7 pages10 11648 J Ajim 20180606 14Stephanie HellenNo ratings yet
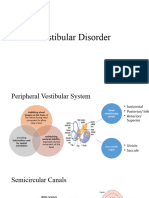
- Vestibular DisorderDocument22 pagesVestibular DisorderSumbal SalikNo ratings yet
- FertilityDocument207 pagesFertilitypmotcNo ratings yet
- June 2023 (v1) (9-1) QP - Paper 4 CAIE Biology IGCSEDocument20 pagesJune 2023 (v1) (9-1) QP - Paper 4 CAIE Biology IGCSEismgilovamunisa150No ratings yet
- Experiment No.9Document7 pagesExperiment No.9ZethBlancada Diesta BarramedaNo ratings yet
- EcosystemDocument61 pagesEcosystemdhitacindyNo ratings yet
- Animal Nutrition PDFDocument26 pagesAnimal Nutrition PDFabdulrehman mughalNo ratings yet
- Textbook: Molecular Biology of The Cell 6th Edition. by Alberts Et AlDocument5 pagesTextbook: Molecular Biology of The Cell 6th Edition. by Alberts Et Al김성한No ratings yet
- Blue. 1 or 2 HoursDocument5 pagesBlue. 1 or 2 HoursAngela ReyesNo ratings yet
- General Psychology Part IDocument107 pagesGeneral Psychology Part Isrbana7025100% (1)
- Pediatric Case History 6 ZsmuDocument4 pagesPediatric Case History 6 ZsmuSagar KhairwalNo ratings yet