You might also like
- LP Cidera KepalaDocument3 pagesLP Cidera KepalafariisakbbarNo ratings yet
- Daftar Pemeriksaan Golongan Darah Dusun Kepuhan 12 Januari 2018Document2 pagesDaftar Pemeriksaan Golongan Darah Dusun Kepuhan 12 Januari 2018fariisakbbarNo ratings yet
- Ipi 195800Document8 pagesIpi 195800Mukhlis HasNo ratings yet
- Assessment and Management of Agitation in Psychiatry Expert ConsensusDocument44 pagesAssessment and Management of Agitation in Psychiatry Expert ConsensusAmi Septia HardiyantiNo ratings yet
- Bahasa InggrisDocument2 pagesBahasa InggrisfariisakbbarNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Genetic Engineering Has Applications in MedicineDocument6 pagesGenetic Engineering Has Applications in Medicineshiv kapilaNo ratings yet
- Future Doctor CCCDocument1 pageFuture Doctor CCCwlshakespeareNo ratings yet
- MotherFirst - Maternity Mental Health Strategy: Building Capacity in SaskatchewanDocument64 pagesMotherFirst - Maternity Mental Health Strategy: Building Capacity in SaskatchewankidSKAN Director100% (1)
- Final Period - Assignment NCM 105Document3 pagesFinal Period - Assignment NCM 105Chester NicoleNo ratings yet
- 129 Accommodative EsotropiaDocument6 pages129 Accommodative EsotropiakarenafiafiNo ratings yet
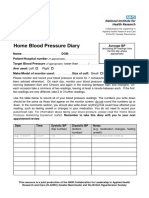
- Home Blood Pressure DiaryDocument2 pagesHome Blood Pressure DiaryCherieNo ratings yet
- HMS-PSG Revenue Maximization Proposal To WV Dept of Health and Human Resources (2012)Document278 pagesHMS-PSG Revenue Maximization Proposal To WV Dept of Health and Human Resources (2012)Rick ThomaNo ratings yet
- Ophthalmology PDFDocument28 pagesOphthalmology PDFKukuh Rizwido PrasetyoNo ratings yet
- Fracturas SubtrocantericasDocument9 pagesFracturas SubtrocantericasPedro Fernando GiraldoNo ratings yet
- LFD Opd-PediaDocument2 pagesLFD Opd-PediaBaccay GeremieNo ratings yet
- Surveillance Procedure PDFDocument4 pagesSurveillance Procedure PDFmonir61No ratings yet
- Essential Elements of Communication in Medical.21 PDFDocument4 pagesEssential Elements of Communication in Medical.21 PDFdr_mksinhaNo ratings yet
- ICU Liberation ABCDEF Bundle Implementation Both Spontaneous Awakening Breathing Trials SBT SATDocument63 pagesICU Liberation ABCDEF Bundle Implementation Both Spontaneous Awakening Breathing Trials SBT SATbejoNo ratings yet
- VA Org Briefing BookDocument59 pagesVA Org Briefing BookJimNo ratings yet
- Diarrhea CareplanDocument6 pagesDiarrhea CareplanAmira Fatmah QuilapioNo ratings yet
- Emotions and Body ChemicalsDocument24 pagesEmotions and Body ChemicalsJanani Anbalagan100% (3)
- Good Posture... Just How Important Is It?: Source: Kansas Chiropractic Foundation WebsiteDocument4 pagesGood Posture... Just How Important Is It?: Source: Kansas Chiropractic Foundation WebsiteJacklynlim LkcNo ratings yet
- Medicolegal Book ContentsDocument5 pagesMedicolegal Book ContentsVirendar Pal SinghNo ratings yet
- Acr 22591Document13 pagesAcr 22591keyla_shineeeNo ratings yet
- Bronchial AsthmaDocument8 pagesBronchial AsthmaBrylle CapiliNo ratings yet
- NCP For Laryngeal CancerDocument5 pagesNCP For Laryngeal CancerMădălina PinciucNo ratings yet
- CT Somatom DefinitionDocument52 pagesCT Somatom DefinitionBharat NandulaNo ratings yet
- Practical Manual On Veterinary Clinical Diagnostic Approach 2157 7579 1000337Document10 pagesPractical Manual On Veterinary Clinical Diagnostic Approach 2157 7579 1000337Shravankumar Gaddi100% (1)
- Geriatric RehabilitationDocument57 pagesGeriatric Rehabilitationrejianil100% (4)
- VIDATOX ® 30 CH EnglishDocument17 pagesVIDATOX ® 30 CH EnglishmusicaNo ratings yet
- Case StudiesDocument17 pagesCase StudiesDamian Maguire100% (4)
- Benign Prostat HiperplasiaDocument17 pagesBenign Prostat HiperplasiahawhawnurNo ratings yet
- Laboratory Medicine Quality IndicatorsDocument14 pagesLaboratory Medicine Quality IndicatorskinnusaraiNo ratings yet
- Course List For The Bachelor of Pharmacy (Honours) - My - UQ - The University of Queensland, AustraliaDocument2 pagesCourse List For The Bachelor of Pharmacy (Honours) - My - UQ - The University of Queensland, AustraliaLy Huyen TranNo ratings yet
- Pre Employment Occupational Health FormDocument7 pagesPre Employment Occupational Health Formlinks2309No ratings yet