You might also like
- Fast Facts: Inflammatory Bowel Disease: Translating the science into compassionate IBD careFrom EverandFast Facts: Inflammatory Bowel Disease: Translating the science into compassionate IBD careNo ratings yet
- Necrotizing EnterocolitisDocument2 pagesNecrotizing EnterocolitisSina AryaNo ratings yet
- Optimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsFrom EverandOptimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsNo ratings yet
- Perks ArticleDocument10 pagesPerks ArticleRangga Duo RamadanNo ratings yet
- Probioticos - Enterocolitis Necrozante en PrematurosDocument7 pagesProbioticos - Enterocolitis Necrozante en PrematurosJuan David Montua ValenciaNo ratings yet
- Acta PaediatricaDocument13 pagesActa PaediatricaDefranky TheodorusNo ratings yet
- 2018 Article 1326Document8 pages2018 Article 1326Mohammad Ziaul KarimNo ratings yet
- The Pathophysiology of Necrotizing Enterocolitis: ObjectivesDocument7 pagesThe Pathophysiology of Necrotizing Enterocolitis: ObjectivesResti Rahmadika AkbarNo ratings yet
- Hollym Necrotizing Enterocolitis - Pathophysiology and Prevention 4Document14 pagesHollym Necrotizing Enterocolitis - Pathophysiology and Prevention 4api-346859104No ratings yet
- Probiotics and Preterm Infants A Position Paper.26 ShareDocument17 pagesProbiotics and Preterm Infants A Position Paper.26 Shareendy tovarNo ratings yet
- Current Knowledge of Necrotizing Enterocolitis in Preterm Infants and The Impact of Different Types of Enteral Nutrition ProductsDocument12 pagesCurrent Knowledge of Necrotizing Enterocolitis in Preterm Infants and The Impact of Different Types of Enteral Nutrition ProductsDana KristalisaNo ratings yet
- Probiotik Clinical Applications in Gastrointestinal DiseaseDocument29 pagesProbiotik Clinical Applications in Gastrointestinal DiseaseDwi Feri HariyantoNo ratings yet
- Clinical NutritionDocument6 pagesClinical NutritionaliyaNo ratings yet
- Probiotics and Prebiotics in Pediatrics, What Is NewDocument5 pagesProbiotics and Prebiotics in Pediatrics, What Is NewJUAN SEBASTIAN AVELLANEDA MARTINEZNo ratings yet
- Early Enteral Feeding and Nosocomial Sepsis in Very Low Birthweight InfantsDocument4 pagesEarly Enteral Feeding and Nosocomial Sepsis in Very Low Birthweight InfantsaripbudiboyNo ratings yet
- 2020 Nutrients Glycosaminoglycans in Protection From EcnDocument20 pages2020 Nutrients Glycosaminoglycans in Protection From EcnMiguel MartinezNo ratings yet
- Probiotic Effects On Late-Onset Sepsis in Very Preterm InfantsDocument23 pagesProbiotic Effects On Late-Onset Sepsis in Very Preterm InfantsyayaseptianaNo ratings yet
- Antiallergic Effects of ProbioticsDocument4 pagesAntiallergic Effects of ProbioticsputrinaraheswariNo ratings yet
- Importance of Maternal Diet 2018Document10 pagesImportance of Maternal Diet 2018Cláudia SilvaNo ratings yet
- Neonatal Necrotizing Enterocolitis: Research and Reports in Neonatology DoveDocument15 pagesNeonatal Necrotizing Enterocolitis: Research and Reports in Neonatology DovedewiswahyuNo ratings yet
- Neonatal Sepsis in The Very Low Birth Weight Preterm Infants: Part 1: Review of Patho-PhysiologyDocument10 pagesNeonatal Sepsis in The Very Low Birth Weight Preterm Infants: Part 1: Review of Patho-PhysiologyjukunkNo ratings yet
- Breastfeeding and The Risk For Diarrhea Morbidity and MortalityDocument12 pagesBreastfeeding and The Risk For Diarrhea Morbidity and MortalityMariam AbdAlkarimNo ratings yet
- Gestational Age, Mode of Birth and Breastmilk Feeding All Influence Acute Early Childhood Gastroenteritis: A Record-Linkage Cohort StudyDocument10 pagesGestational Age, Mode of Birth and Breastmilk Feeding All Influence Acute Early Childhood Gastroenteritis: A Record-Linkage Cohort Studynavali rahmaNo ratings yet
- NIH Public Access: Gastrointestinal Microbiome Signatures of Pediatric Patients With Irritable Bowel SyndromeDocument19 pagesNIH Public Access: Gastrointestinal Microbiome Signatures of Pediatric Patients With Irritable Bowel SyndromesebaspezoaNo ratings yet
- Norkhafizah, S, Norsa'adah, BDocument3 pagesNorkhafizah, S, Norsa'adah, BWindi 17090No ratings yet
- Article OropharyngealDocument14 pagesArticle OropharyngealMelissa IllidgeNo ratings yet
- Impact of Maternal Probiotic Supplemented Dietary Counselling On Pregnancy Outcome and Prenatal and Postnatal Growth A Double Blind Placebo Controlled StudyDocument8 pagesImpact of Maternal Probiotic Supplemented Dietary Counselling On Pregnancy Outcome and Prenatal and Postnatal Growth A Double Blind Placebo Controlled Studytami ariyasraNo ratings yet
- Estacion EsDocument12 pagesEstacion EsLuis Quito CaroNo ratings yet
- Prebiotic Effect in The Healthy Infant - Recent Update: Yvan - Vandenplas@uzbrussel - BeDocument53 pagesPrebiotic Effect in The Healthy Infant - Recent Update: Yvan - Vandenplas@uzbrussel - BegazalidjawadNo ratings yet
- The Effect of Probiotics in Prevention of Necrotising Enterocolitis in Preterm Neonates in Comparison With Control GroupDocument4 pagesThe Effect of Probiotics in Prevention of Necrotising Enterocolitis in Preterm Neonates in Comparison With Control GroupchachaNo ratings yet
- Antibiotics, Pediatric Dysbiosis, and DiseaseREVISADODocument12 pagesAntibiotics, Pediatric Dysbiosis, and DiseaseREVISADOEsbe GabyNo ratings yet
- Agus K LarobuDocument9 pagesAgus K LarobuAgus LarobuNo ratings yet
- The Role of Maternal Breast Milk in Preventing Infantile DiarrheaDocument16 pagesThe Role of Maternal Breast Milk in Preventing Infantile Diarrheamaria putriNo ratings yet
- JN 212308Document8 pagesJN 212308Ivhajannatannisa KhalifatulkhusnulkhatimahNo ratings yet
- Probiotics For The Prevention of Pediatric Antibiotic-Associated Diarrhea (Review)Document4 pagesProbiotics For The Prevention of Pediatric Antibiotic-Associated Diarrhea (Review)EvelynRuizNo ratings yet
- Neonatal Necrotizing Enterocolitis - Pathology and Pathogenesis - UpToDateDocument21 pagesNeonatal Necrotizing Enterocolitis - Pathology and Pathogenesis - UpToDateSamuel Idrogo AlfaroNo ratings yet
- Clinical Indications ForDocument7 pagesClinical Indications Forronywijaya7No ratings yet
- Pro Bio Tics Future DirectionsDocument3 pagesPro Bio Tics Future Directionstuphong9988No ratings yet
- TP 08 03 212Document15 pagesTP 08 03 212Hendro SihalohoNo ratings yet
- Review Article: Choice and Duration of Antimicrobial Therapy For Neonatal Sepsis and MeningitisDocument10 pagesReview Article: Choice and Duration of Antimicrobial Therapy For Neonatal Sepsis and MeningitisjessicacookNo ratings yet
- Review Article: Probiotics and Gastrointestinal InfectionsDocument11 pagesReview Article: Probiotics and Gastrointestinal InfectionsFarid FergianNo ratings yet
- Probiotics: Kathi J Kemper, MD, MPH Wake Forest University School of MedicineDocument36 pagesProbiotics: Kathi J Kemper, MD, MPH Wake Forest University School of MedicinevinniejulianaNo ratings yet
- Antimicrobial Therapy and Late Onset SepsisDocument10 pagesAntimicrobial Therapy and Late Onset SepsisKendy LópezNo ratings yet
- Necrotizing Enterocolitis in Newborns: Update in Pathophysiology and Newly Emerging Therapeutic StrategiesDocument9 pagesNecrotizing Enterocolitis in Newborns: Update in Pathophysiology and Newly Emerging Therapeutic Strategiesemilly vidyaNo ratings yet
- RHL - WHO Recommendation On Intrapartum Antibiotic Administration To Women With Group B Streptococcus (GBS) Colonization For Prevention of Early Neonatal GBS Infection. - 2018-04-04Document5 pagesRHL - WHO Recommendation On Intrapartum Antibiotic Administration To Women With Group B Streptococcus (GBS) Colonization For Prevention of Early Neonatal GBS Infection. - 2018-04-04Letícia ZanotelliNo ratings yet
- Dyq 030Document10 pagesDyq 030Marlintan Sukma AmbarwatiNo ratings yet
- Probiotics in Adolescent Prediabetes: A Pilot RCT On Glycemic Control and Intestinal BacteriomeDocument14 pagesProbiotics in Adolescent Prediabetes: A Pilot RCT On Glycemic Control and Intestinal BacteriomeKarina EkawidyaniNo ratings yet
- Jurnal 7Document5 pagesJurnal 7aliyaNo ratings yet
- Oral Polio Influences Immune Response To BCG VaccinationDocument9 pagesOral Polio Influences Immune Response To BCG Vaccinationromeoenny4154No ratings yet
- Accepted Manuscript: Genomics, Proteomics & BioinformaticsDocument34 pagesAccepted Manuscript: Genomics, Proteomics & BioinformaticsDiogoNo ratings yet
- Early Life Formula Feeding Is Associated With Infant - 2022 - The American JourDocument15 pagesEarly Life Formula Feeding Is Associated With Infant - 2022 - The American JourneurotransformacaoNo ratings yet
- IBFAN Asia Position Statement On HIV and Infant Feeding (October 2008)Document6 pagesIBFAN Asia Position Statement On HIV and Infant Feeding (October 2008)Anil MishraNo ratings yet
- Efficacy and Safety of Fluconazole Prophylaxis in Extremely Low Birth Weight Infants: Multicenter Pre-Post Cohort StudyDocument10 pagesEfficacy and Safety of Fluconazole Prophylaxis in Extremely Low Birth Weight Infants: Multicenter Pre-Post Cohort StudyAnry UmarNo ratings yet
- Strepto 2020Document12 pagesStrepto 2020Jordana NahsanNo ratings yet
- Early Total Enteral Feeding in Stable Very Low Birth Weight Infants: A Before and After StudyDocument7 pagesEarly Total Enteral Feeding in Stable Very Low Birth Weight Infants: A Before and After StudySupriya M A SuppiNo ratings yet
- Probiotics: Complementary and Alternative Medicine: A New SeriesDocument3 pagesProbiotics: Complementary and Alternative Medicine: A New SeriesKarol CañasNo ratings yet
- Latihan. Journal Appraisal - OriginalDocument8 pagesLatihan. Journal Appraisal - Originalindriani putriNo ratings yet
- Vesterlund Et Al, 2007 - Safety Assessment of Lactobacillus Strains PDFDocument7 pagesVesterlund Et Al, 2007 - Safety Assessment of Lactobacillus Strains PDFDanilo SilvaNo ratings yet
- Infecciones NeonatalesDocument23 pagesInfecciones NeonatalesAlejandra MedinaNo ratings yet
- Pro Bio TicsDocument9 pagesPro Bio TicsRenka Joy AbadNo ratings yet
- Drug AntagonismDocument9 pagesDrug AntagonismSeptaPratamaAptNo ratings yet
- Cover Kebijakan MutuDocument1 pageCover Kebijakan MutuSeptaPratamaAptNo ratings yet
- PlagiarismDocument33 pagesPlagiarismMahrukh BaigNo ratings yet
- PHARMACOLOGY-introDocument18 pagesPHARMACOLOGY-introSeptaPratamaAptNo ratings yet
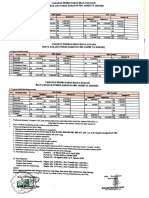
- Biaya Kuliah PMB 2020Document1 pageBiaya Kuliah PMB 2020SeptaPratamaAptNo ratings yet
- Principle of Drug ActionDocument15 pagesPrinciple of Drug ActionSeptaPratamaAptNo ratings yet
- Stok Opname 28 Feb (Gudang) - 1Document144 pagesStok Opname 28 Feb (Gudang) - 1SeptaPratamaAptNo ratings yet
- Antimicrobial Stewardship PDFDocument37 pagesAntimicrobial Stewardship PDFSeptaPratamaAptNo ratings yet
- Order Obat 2Document4 pagesOrder Obat 2SeptaPratamaAptNo ratings yet
- Stok Opname 28 Feb (Gudang) - 1Document144 pagesStok Opname 28 Feb (Gudang) - 1SeptaPratamaAptNo ratings yet
- Beta LactamDocument14 pagesBeta LactamSeptaPratamaAptNo ratings yet
- Infographic Antimicrobial Resistance 20140430 PDFDocument1 pageInfographic Antimicrobial Resistance 20140430 PDFMarkus AbiogNo ratings yet
- Drug Dose Adjustment in Chronic Renal Diseases: Medicine UpdateDocument7 pagesDrug Dose Adjustment in Chronic Renal Diseases: Medicine UpdateSeptaPratamaAptNo ratings yet
- Eligible Study Programmes by Partners Final1701191426Document130 pagesEligible Study Programmes by Partners Final1701191426Eko Bayu AjiNo ratings yet
- Antibiotics 170308134011 PDFDocument81 pagesAntibiotics 170308134011 PDFSeptaPratamaAptNo ratings yet
- Ang 2 PDFDocument12 pagesAng 2 PDFSeptaPratamaAptNo ratings yet
- Antimicrobial StewardshipDocument37 pagesAntimicrobial StewardshipSeptaPratamaAptNo ratings yet
- E1304amcp - 11.15.13 Final JMCP VersionDocument22 pagesE1304amcp - 11.15.13 Final JMCP VersionSeptaPratamaAptNo ratings yet
- I Don't KnowDocument1 pageI Don't KnowSeptaPratamaAptNo ratings yet
- No. 018/UGM/OGV/EP/XIX/2017: AIESEC in Universitas Gadjah MadaDocument2 pagesNo. 018/UGM/OGV/EP/XIX/2017: AIESEC in Universitas Gadjah MadaSeptaPratamaAptNo ratings yet
- E1304amcp - 11.15.13 Final JMCP VersionDocument22 pagesE1304amcp - 11.15.13 Final JMCP VersionSeptaPratamaAptNo ratings yet
- Drug-Induced Nephrotoxicity: Cynthia A. Naughton, Pharmd, BCPS, North Dakota State University College of PharmacyDocument8 pagesDrug-Induced Nephrotoxicity: Cynthia A. Naughton, Pharmd, BCPS, North Dakota State University College of PharmacyAbdur Rachman Ba'abdullahNo ratings yet
- Invoice Septa UnajaDocument1 pageInvoice Septa UnajaSeptaPratamaAptNo ratings yet
- WHO - Indoor Air PollutionDocument484 pagesWHO - Indoor Air PollutionCosmo Deus100% (2)
- Denah ApotekDocument1 pageDenah ApotekSeptaPratamaAptNo ratings yet
- Itinerary Visit ParisDocument1 pageItinerary Visit ParisSeptaPratamaAptNo ratings yet
- SSM Application SummaryDocument61 pagesSSM Application SummarySeptaPratamaAptNo ratings yet
- 3rd LabDocument47 pages3rd LabUmair GulzarNo ratings yet
- 1 s2.0 S0378427416329381 MainDocument1 page1 s2.0 S0378427416329381 MainSeptaPratamaAptNo ratings yet
- 330A 2018docDocument20 pages330A 2018docDavid MendozaNo ratings yet
- MIS ProjectDocument12 pagesMIS ProjectDuc Anh67% (3)
- CBR Bahasa Inggris Fisika Kelompok 1Document9 pagesCBR Bahasa Inggris Fisika Kelompok 1Ryan SianiparNo ratings yet
- The Right MindDocument8 pagesThe Right Mindwaltor makuvireNo ratings yet
- Jaw Crusher Kinematics Simulation and AnalysisDocument5 pagesJaw Crusher Kinematics Simulation and AnalysisInternational Journal of Research in Engineering and ScienceNo ratings yet
- Factors Influencing The PerceptionDocument1 pageFactors Influencing The PerceptionTinesh Kumar100% (1)
- Training Needs in Facilities Management Zaharah Manaf 2005Document11 pagesTraining Needs in Facilities Management Zaharah Manaf 2005Anonymous dmYc1M4uNo ratings yet
- President Uhuru Kenyatta's Speech During The Kenya@50 Celebrations at Uhuru Gardens, Nairobi On The Mid-Night of 12th December, 2013Document3 pagesPresident Uhuru Kenyatta's Speech During The Kenya@50 Celebrations at Uhuru Gardens, Nairobi On The Mid-Night of 12th December, 2013State House KenyaNo ratings yet
- Dallas Baptist University Writing Center: Narrative EssayDocument3 pagesDallas Baptist University Writing Center: Narrative EssayumagandhiNo ratings yet
- Introductory Econometrics A Modern Approach Solutions Manual PDFDocument9 pagesIntroductory Econometrics A Modern Approach Solutions Manual PDFAnonymous bzcYj42Ain0% (2)
- Access 1 Nahwu PDFDocument234 pagesAccess 1 Nahwu PDFAmru-Rizal RazaniNo ratings yet
- Tort of NegligenceDocument2 pagesTort of NegligenceYANZHUNo ratings yet
- From Carpathian To PindusDocument482 pagesFrom Carpathian To Pindussc0ril0100% (5)
- Ed 2 Module 8 1Document5 pagesEd 2 Module 8 1Jimeniah Ignacio RoyoNo ratings yet
- G.R. No. 92735 Monarch V CA - DigestDocument2 pagesG.R. No. 92735 Monarch V CA - DigestOjie Santillan100% (1)
- Test 2A AP StatisticsDocument5 pagesTest 2A AP StatisticssnarkjazzoNo ratings yet
- Visual Development Milestones and Visual Acuity Assessment in ChildrenDocument2 pagesVisual Development Milestones and Visual Acuity Assessment in ChildrenNikhil Maha DevanNo ratings yet
- Science - G8 - Q1 - Week 4Document48 pagesScience - G8 - Q1 - Week 4Angelito MadesNo ratings yet
- y D Starter PDFDocument13 pagesy D Starter PDFnazar750No ratings yet
- Buad 306 HW 2Document4 pagesBuad 306 HW 2AustinNo ratings yet
- Sorrows of A Trophy WifeDocument786 pagesSorrows of A Trophy WifeAngel MilanNo ratings yet
- DECLAMATIONDocument19 pagesDECLAMATIONJohn Carlos Wee67% (3)
- EndomytosisDocument8 pagesEndomytosisBlackbeetleNo ratings yet
- The Importance of Instructional MaterialDocument3 pagesThe Importance of Instructional MaterialJheramae SegoviaNo ratings yet
- 4 5 and 6 - Approaches To HR MeasurementDocument14 pages4 5 and 6 - Approaches To HR MeasurementRahul RaoNo ratings yet
- 8035-Article Text-59635-1-10-20190329Document4 pages8035-Article Text-59635-1-10-20190329Hesti RahmadatiNo ratings yet
- Resilient Modulus of Hot-Mix Asphalt Gap Graded With Waste Rubber Tire AdditivesDocument10 pagesResilient Modulus of Hot-Mix Asphalt Gap Graded With Waste Rubber Tire Additivesdanang abdilahNo ratings yet
- After The Banquet - Yukio MishimaDocument171 pagesAfter The Banquet - Yukio Mishimalazar10plusNo ratings yet
- Martin Luther King. Answer KeyDocument1 pageMartin Luther King. Answer KeyOleg MuhendisNo ratings yet
- Adenariwo AdepojuDocument225 pagesAdenariwo AdepojustarykltNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (28)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (2)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (4)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (58)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (45)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)