You might also like
- Common Issues When Caring for Seniors: The Aging Process Cognitive DeclineFrom EverandCommon Issues When Caring for Seniors: The Aging Process Cognitive DeclineNo ratings yet
- 363 Dementia AwarnessDocument4 pages363 Dementia AwarnessCatalin MinascurtaNo ratings yet
- Minds Fading Away : Alzheimer's And Dementia GuideFrom EverandMinds Fading Away : Alzheimer's And Dementia GuideRating: 5 out of 5 stars5/5 (1)
- Done By: Mostafa Grade: 10B Bio Teacher: Mr. Kamel: What Is Alzheimer's Disease?Document18 pagesDone By: Mostafa Grade: 10B Bio Teacher: Mr. Kamel: What Is Alzheimer's Disease?Mostafa BayoumyNo ratings yet
- Running Head: Do People Get Memory Loss in Old-Age? 1Document8 pagesRunning Head: Do People Get Memory Loss in Old-Age? 1Pham DatNo ratings yet
- Alzheimer's Disease: Pre Dementia Early Moderate AdvancedDocument7 pagesAlzheimer's Disease: Pre Dementia Early Moderate AdvancedNavjot BrarNo ratings yet
- Agepage: Forgetfulness: Knowing When To Ask For HelpDocument12 pagesAgepage: Forgetfulness: Knowing When To Ask For HelpJohnfoxy JfoxyNo ratings yet
- A Simple Guide to Dementia and Alzheimer's DiseasesFrom EverandA Simple Guide to Dementia and Alzheimer's DiseasesRating: 5 out of 5 stars5/5 (1)
- Caring for someone with dementia guideDocument45 pagesCaring for someone with dementia guideTony Abott100% (3)
- Alzheimer's Disease: A Guide to Symptoms, Causes, Stages and TreatmentsDocument16 pagesAlzheimer's Disease: A Guide to Symptoms, Causes, Stages and TreatmentsKathleen DiangoNo ratings yet
- A Simple Guide to Dementia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Dementia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Dementia GeriaDocument3 pagesDementia GeriaIan Lusay OfendoreyesNo ratings yet
- Products & Services: Book: Mayo Clinic Guide To Stress-Free LivingDocument10 pagesProducts & Services: Book: Mayo Clinic Guide To Stress-Free LivingoliviaNo ratings yet
- Preface: Psychoanalytic Psychotherapy: in Its Purest Form, Two Types of ProblemsDocument18 pagesPreface: Psychoanalytic Psychotherapy: in Its Purest Form, Two Types of ProblemsLamanta JazeNo ratings yet
- A Simple Guide to Mild Cognitive Impairment, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Mild Cognitive Impairment, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Mild Cognitive Impairment FactsheetDocument6 pagesMild Cognitive Impairment FactsheetJoasVinsensiusDavianNo ratings yet
- Introduction - Alzheimer's DiseaseDocument9 pagesIntroduction - Alzheimer's Diseasepriya swathiNo ratings yet
- What Is DementiaDocument5 pagesWhat Is DementiaIuly ManacNo ratings yet
- Understanding Dementia: Causes, Symptoms and TypesDocument3 pagesUnderstanding Dementia: Causes, Symptoms and TypesSWAPNILNo ratings yet
- Diseases & Disorders Dementia, Alzheimer's DiseaseDocument11 pagesDiseases & Disorders Dementia, Alzheimer's DiseaseAngela DepedroNo ratings yet
- Mental Changes in AgingDocument4 pagesMental Changes in AgingPRINTDESK by DanNo ratings yet
- Basics of Alzheimer's Disease: What It Is and What You Can DoDocument32 pagesBasics of Alzheimer's Disease: What It Is and What You Can DoKarachibreezeNo ratings yet
- Alzheimer'S Disease: Miss Sana HanifDocument27 pagesAlzheimer'S Disease: Miss Sana HanifDr-umar AliNo ratings yet
- DementiaDocument13 pagesDementiakololll lllknNo ratings yet
- Alzheimer's and Dementia BasicsDocument2 pagesAlzheimer's and Dementia BasicsVictor Alejandro Larios SalazarNo ratings yet
- Dementia: What Is The Difference Between Alzheimer's Disease and Dementia?Document2 pagesDementia: What Is The Difference Between Alzheimer's Disease and Dementia?anuchNo ratings yet
- A Simple Guide to Types of Dementia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Types of Dementia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Compare Myelomeningocele With Cerebral Palsy in Terms of Etiology and Effects On Motor Functioning and CommunicationDocument4 pagesCompare Myelomeningocele With Cerebral Palsy in Terms of Etiology and Effects On Motor Functioning and CommunicationZulma MunizNo ratings yet
- Seniors with Age-Related Memory Decline: A Caregiver's GuideFrom EverandSeniors with Age-Related Memory Decline: A Caregiver's GuideNo ratings yet
- Bio InvestigatoryDocument12 pagesBio InvestigatorySonakshi BadlaniNo ratings yet
- Alzheimer Cover Page (Hard Cover)Document21 pagesAlzheimer Cover Page (Hard Cover)seanfaria100% (1)
- Alzheimer's Disease Research PaperDocument24 pagesAlzheimer's Disease Research Papershayne86% (22)
- Science FairDocument8 pagesScience FairmigrinNo ratings yet
- AlzheimerDocument11 pagesAlzheimerSoniya G08No ratings yet
- Alzheimer's Disease ResearchDocument61 pagesAlzheimer's Disease ResearchshayneNo ratings yet
- Alzheimer's Disease Fact Sheet: Symptoms DementiaDocument16 pagesAlzheimer's Disease Fact Sheet: Symptoms DementiaJovelyn Morales JosolNo ratings yet
- Know DementiaDocument2 pagesKnow Dementiapaulacabading.pcNo ratings yet
- The Basics of Alzheimer's Disease: Dipil PatelDocument15 pagesThe Basics of Alzheimer's Disease: Dipil Patelgore-patelNo ratings yet
- Alzheimer's Definition ExplainedDocument8 pagesAlzheimer's Definition ExplainedShuhada Abu HassanNo ratings yet
- Alzheimer's DiseaseDocument20 pagesAlzheimer's DiseaseHariharanPillaiNo ratings yet
- The alzheimer's caregiver & families guide: Coping with alzheimers disease, through the stages, including prevention, diet, safety to conventional & alternative healthcare optionsFrom EverandThe alzheimer's caregiver & families guide: Coping with alzheimers disease, through the stages, including prevention, diet, safety to conventional & alternative healthcare optionsNo ratings yet
- What Is DementiaDocument24 pagesWhat Is DementiaJorey QuietaNo ratings yet
- Case Study On DementiaDocument9 pagesCase Study On Dementiatatiana garrovillasNo ratings yet
- What Is Cognitive Impairmenwhat Is Cognitive Impairment?Document5 pagesWhat Is Cognitive Impairmenwhat Is Cognitive Impairment?clccornerNo ratings yet
- Biology Project File Alzheimer: Akshita AgrawalDocument15 pagesBiology Project File Alzheimer: Akshita AgrawalAkshita100% (1)
- Alzheimer DiseaseDocument2 pagesAlzheimer DiseaseRacines Christine Kaye 3A IRREG.No ratings yet
- Alzheimer Disease: A Major Public Health ConcernDocument6 pagesAlzheimer Disease: A Major Public Health ConcerndineshhissarNo ratings yet
- DementiaDocument6 pagesDementiaRoci ArceNo ratings yet
- Thesis - Diagnosis and Treatment of Alzheimer?s Disease - Current CDocument33 pagesThesis - Diagnosis and Treatment of Alzheimer?s Disease - Current CE.Kishore KumarNo ratings yet
- Alzheimer'sDocument2 pagesAlzheimer'smarishkabegheladzeNo ratings yet
- Alzheimer's Disease Causes, Symptoms, and TreatmentDocument4 pagesAlzheimer's Disease Causes, Symptoms, and Treatmentgamecockusc1992No ratings yet
- DementiaDocument3 pagesDementiaJOSH MATTHEW C. LUNZAGANo ratings yet
- Alzheimer’s Society factsheet 458: The progression of Alzheimer’s disease and other dementiasFrom EverandAlzheimer’s Society factsheet 458: The progression of Alzheimer’s disease and other dementiasNo ratings yet
- Alzheimer's Disease Fact SheetDocument6 pagesAlzheimer's Disease Fact SheetInternational Business Times100% (2)
- Role of Sadhana in EnlightenmentDocument2 pagesRole of Sadhana in EnlightenmentIYERBKNo ratings yet
- Are All Angiotensin Receptor Blockers The Same?Document37 pagesAre All Angiotensin Receptor Blockers The Same?IYERBKNo ratings yet
- List of The Greatest Indian NovelsDocument9 pagesList of The Greatest Indian NovelsIYERBKNo ratings yet
- Delicious Dark Greens RecipesDocument8 pagesDelicious Dark Greens RecipesIYERBKNo ratings yet
- Wallpaper Selection GuideDocument4 pagesWallpaper Selection GuideIYERBKNo ratings yet
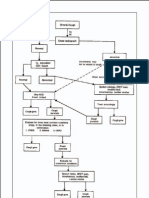
- Chronic Cough - FLOWDocument3 pagesChronic Cough - FLOWIYERBKNo ratings yet
- Aids Malaria Drugs ChartDocument2 pagesAids Malaria Drugs ChartIYERBKNo ratings yet
- Ida SlidesDocument47 pagesIda SlidesIYERBKNo ratings yet
- Cough AlgorithmsDocument2 pagesCough AlgorithmsIYERBK100% (2)
- RTI Chart AdultDocument1 pageRTI Chart AdultIYERBK100% (1)
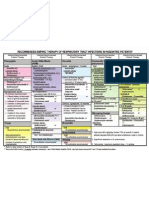
- Anti Infectives Guide For AdultsDocument5 pagesAnti Infectives Guide For AdultsIYERBK100% (1)
- Pneumonia GuidelinesDocument4 pagesPneumonia GuidelinesIYERBK100% (3)
- Rti Aadults AlgorithmDocument2 pagesRti Aadults AlgorithmIYERBKNo ratings yet
- RTI Chart ChildDocument1 pageRTI Chart ChildIYERBKNo ratings yet
- Cap AlgorithmDocument1 pageCap AlgorithmIYERBKNo ratings yet
- Uti AlgorithmDocument1 pageUti AlgorithmIYERBK100% (2)
- STD Treatment ChartDocument5 pagesSTD Treatment ChartIYERBK100% (1)
- Constipation AlgorithmDocument1 pageConstipation AlgorithmIYERBKNo ratings yet
- A.1. Community-Acquired: Use Antibiotics JudiciouslyDocument33 pagesA.1. Community-Acquired: Use Antibiotics JudiciouslymaxgroovesNo ratings yet
- Analysis of Heavy Metals Concentration in Landfill Soil IJERTV8IS120019Document2 pagesAnalysis of Heavy Metals Concentration in Landfill Soil IJERTV8IS120019Eustache NIJEJENo ratings yet
- Role of Family and Society in The Rehabiloitation of Offenders PDFDocument4 pagesRole of Family and Society in The Rehabiloitation of Offenders PDFDevlika DasNo ratings yet
- Gebauer 2012Document26 pagesGebauer 2012Seán GallagherNo ratings yet
- Ignition System Spark Test DiagnosisDocument24 pagesIgnition System Spark Test DiagnosisMohamed l'Amine75% (4)
- EP Series User Manual PDFDocument40 pagesEP Series User Manual PDFa.elwahabNo ratings yet
- Book 1Document94 pagesBook 1JOHNNo ratings yet
- Copia de Tissue Response To Dental CariesDocument7 pagesCopia de Tissue Response To Dental Cariesjorefe12No ratings yet
- GTT Module 5Document156 pagesGTT Module 5ABDULRAHIMAN RAJEKHANNo ratings yet
- Human Capital FormationDocument9 pagesHuman Capital Formationtannu singh67% (6)
- Gate Installation ReportDocument3 pagesGate Installation ReportKumar AbhishekNo ratings yet
- Ic Audio Mantao TEA2261Document34 pagesIc Audio Mantao TEA2261EarnestNo ratings yet
- Q1 Tle 4 (Ict)Document34 pagesQ1 Tle 4 (Ict)Jake Role GusiNo ratings yet
- Intake Sheet SampleDocument1 pageIntake Sheet SampleRochelleNo ratings yet
- TDS Versimax HD4 15W40Document1 pageTDS Versimax HD4 15W40Amaraa DNo ratings yet
- Arp0108 2018Document75 pagesArp0108 2018justin.kochNo ratings yet
- Maual de Servicio TV LG 32lf15r-MaDocument31 pagesMaual de Servicio TV LG 32lf15r-MaJaime E FernandezNo ratings yet
- Đề cương ôn tập tiếng anh 9Document28 pagesĐề cương ôn tập tiếng anh 9Nguyễn HoaNo ratings yet
- Nicenstripy Gardening Risk AssessmentDocument38 pagesNicenstripy Gardening Risk AssessmentVirta Nisa100% (1)
- Aplikasi Berbagai Jenis Media Dan ZPT Terhadap Aklimatisasi Anggrek VandaDocument15 pagesAplikasi Berbagai Jenis Media Dan ZPT Terhadap Aklimatisasi Anggrek VandaSihonoNo ratings yet
- New930e-4se Ceam031503 930e4se Omm A31937 Up PDFDocument273 pagesNew930e-4se Ceam031503 930e4se Omm A31937 Up PDFSergelen SakhyabazarNo ratings yet
- FINALS REVIEWER ENVI ENGG Topic 1Document8 pagesFINALS REVIEWER ENVI ENGG Topic 1As ReNo ratings yet
- NLOG GS PUB 1580 VGEXP-INT3-GG-RPT-0001.00 P11-06 Geological FWRDocument296 pagesNLOG GS PUB 1580 VGEXP-INT3-GG-RPT-0001.00 P11-06 Geological FWRAhmed GharbiNo ratings yet
- 01 - 01 - SK10 - JXNipponDocument1 page01 - 01 - SK10 - JXNipponredevils86No ratings yet
- Completed Manuscript 1 5Document52 pagesCompleted Manuscript 1 5SAMANTHA LACABANo ratings yet
- Funds Flow Statement ExplainedDocument76 pagesFunds Flow Statement Explainedthella deva prasad0% (1)
- 10059-DC-K-01-A Design BasisDocument34 pages10059-DC-K-01-A Design BasisAnonymous RvIgDUNo ratings yet
- The Impact of StressDocument3 pagesThe Impact of StressACabalIronedKryptonNo ratings yet
- FileDocument284 pagesFileJesse GarciaNo ratings yet
- Dip Obst (SA) Past Papers - 2020 1st Semester 1-6-2023Document1 pageDip Obst (SA) Past Papers - 2020 1st Semester 1-6-2023Neo Latoya MadunaNo ratings yet
- ABSCESSDocument35 pagesABSCESSlax prajapatiNo ratings yet