You might also like
- HAES LimitationsDocument5 pagesHAES LimitationsJes BakerNo ratings yet
- Professional PaperDocument20 pagesProfessional Paperapi-242376719No ratings yet
- Weight Science: Evaluating The Evidence For A Paradigm ShiftDocument13 pagesWeight Science: Evaluating The Evidence For A Paradigm ShiftJes BakerNo ratings yet
- HAES FACT SHEET SM Rev 6 6 10Document2 pagesHAES FACT SHEET SM Rev 6 6 10hadyshaNo ratings yet
- Impact of Non-Diet Approaches On Attitu... D Health Outcomes - A Systematic ReviewDocument14 pagesImpact of Non-Diet Approaches On Attitu... D Health Outcomes - A Systematic ReviewJes BakerNo ratings yet
- Review Article Relationships Between Intuitive Eating and Health Indicators Literature ReviewDocument10 pagesReview Article Relationships Between Intuitive Eating and Health Indicators Literature ReviewYasmim CronembergerNo ratings yet
- Snapshot NCP Step 3 Nutrition Intervention-1Document1 pageSnapshot NCP Step 3 Nutrition Intervention-1api-250924915No ratings yet
- Nutrition Care Process and Model UpdateDocument12 pagesNutrition Care Process and Model UpdateRoberto Sedano JiménezNo ratings yet
- Role of DieticianDocument18 pagesRole of DieticianAnju RaniNo ratings yet
- Feeding and Eating Disorder Review LectureDocument4 pagesFeeding and Eating Disorder Review LectureMane SharNo ratings yet
- Is FOOD Your Biggest Challenge To Losing Weight?Document18 pagesIs FOOD Your Biggest Challenge To Losing Weight?nicoleNo ratings yet
- Mindful Eating Weight To WellbeingDocument14 pagesMindful Eating Weight To WellbeingCitra AyuNo ratings yet
- PDF Nutrition CM 1 CU 1 LEC WEEK 1Document27 pagesPDF Nutrition CM 1 CU 1 LEC WEEK 1Zharm MayNo ratings yet
- Fad Diets Do Not Promote Long Term Weight LossDocument7 pagesFad Diets Do Not Promote Long Term Weight Lossapi-582244166No ratings yet
- IE Talk 2020 PDFDocument46 pagesIE Talk 2020 PDFTatyana AsenovaNo ratings yet
- Nutrition and Dietary Pattern: Chap-5Document41 pagesNutrition and Dietary Pattern: Chap-5Imad AgarwalNo ratings yet
- NCPT For EALDocument61 pagesNCPT For EALAsri SubarjatiNo ratings yet
- Saudi Guideline Prevention Management Overweight Obesity 2022Document82 pagesSaudi Guideline Prevention Management Overweight Obesity 2022إكرام النايبNo ratings yet
- Case Study Childhood OverweightDocument6 pagesCase Study Childhood Overweightmaalaka100% (1)
- Why Am I Binge EatingDocument3 pagesWhy Am I Binge EatingDeep SpoonNo ratings yet
- Vitality Weight Management Guide ENDocument15 pagesVitality Weight Management Guide ENUnkown Unkown100% (1)
- Exam 3Document6 pagesExam 3Vivechana ParajuliNo ratings yet
- Nutrition in Health and Illness: For 2 Yr Nursing StudentsDocument46 pagesNutrition in Health and Illness: For 2 Yr Nursing StudentsGizachew Asimare100% (1)
- Health Assessment AssignmentDocument8 pagesHealth Assessment Assignmentapi-314827222100% (1)
- Nutritional AccessmentDocument4 pagesNutritional AccessmentSaher YasinNo ratings yet
- Book Review HaesDocument7 pagesBook Review Haesapi-527663434No ratings yet
- Rumination DisorderDocument15 pagesRumination DisorderNAMRATA_NARANG54880% (1)
- Pes Statements SamplesDocument19 pagesPes Statements SamplesJennie ManobanNo ratings yet
- Brochure HMS LIME 12-04-22 V21Document14 pagesBrochure HMS LIME 12-04-22 V21i10 Sport PlusNo ratings yet
- Nutrition Care Process: Problem: Diagnostic Label (Term and Code) Etiology: Related Factors Contributing ToDocument1 pageNutrition Care Process: Problem: Diagnostic Label (Term and Code) Etiology: Related Factors Contributing ToBern NerquitNo ratings yet
- Nutrition FactsDocument4 pagesNutrition Factsnajie talonNo ratings yet
- Psychology and NutritionDocument2 pagesPsychology and NutritionalyNo ratings yet
- Nutritional Biochemistry For Undergraduates - 102524Document13 pagesNutritional Biochemistry For Undergraduates - 102524Amal MohammedNo ratings yet
- Understanding: Body Dysmorphic DisorderDocument14 pagesUnderstanding: Body Dysmorphic DisordervivienNo ratings yet
- Eating Disorders: 1. Anorexia NervosaDocument7 pagesEating Disorders: 1. Anorexia NervosaPaul Vincent LauretaNo ratings yet
- Human Nutrition QuizDocument6 pagesHuman Nutrition QuizMattMattTv JapanNo ratings yet
- Adult Weight Management ToolkitDocument4 pagesAdult Weight Management ToolkitAmany Salama67% (3)
- Libro TCA - ANDDocument228 pagesLibro TCA - ANDCarpetas PSicologiaNo ratings yet
- Binge Eating Disorder (Niddk)Document6 pagesBinge Eating Disorder (Niddk)rodolfo_green_1No ratings yet
- Eating Disorders 1Document46 pagesEating Disorders 1Heba_Al_KhozaeNo ratings yet
- 2006 Vegetarian Diets - Nutritional Considerations For AthletesDocument14 pages2006 Vegetarian Diets - Nutritional Considerations For AthletesAni Fran SolarNo ratings yet
- The Role of Nutrition For Pressure Ulcer.7Document14 pagesThe Role of Nutrition For Pressure Ulcer.7Keyser SozeNo ratings yet
- Nutrition Basics Student-CompressedDocument164 pagesNutrition Basics Student-CompressedKatieNo ratings yet
- From The Academy: Standards of PracticeDocument73 pagesFrom The Academy: Standards of Practicejustin babiNo ratings yet
- Process Nutrition Care Terminology (NCPT) : R GHTDocument64 pagesProcess Nutrition Care Terminology (NCPT) : R GHTnoviananurhanifahNo ratings yet
- MNT 1 DM Case Study Due 11 29 2016Document3 pagesMNT 1 DM Case Study Due 11 29 2016api-340581896No ratings yet
- Nutritional Diagnosis PresentationDocument27 pagesNutritional Diagnosis PresentationEddie ChenNo ratings yet
- Scale Development - Diabetes ScaleDocument63 pagesScale Development - Diabetes ScalehadiyudhaNo ratings yet
- APPETITE: Physiological and Neurobiological AspectsDocument8 pagesAPPETITE: Physiological and Neurobiological AspectsTamara Souza RossiNo ratings yet
- Nutritional Care ProcessDocument17 pagesNutritional Care ProcessAlison OfeNo ratings yet
- Letter To Treatment ProviderDocument1 pageLetter To Treatment ProviderAshley McGuffinNo ratings yet
- Obesity KetogenicDocument16 pagesObesity KetogenicReza Firsandaya MalikNo ratings yet
- 2018 Nutrition Intervention SnapshotDocument1 page2018 Nutrition Intervention SnapshotIrhamna Fauziah100% (1)
- Cole Kelby Nutrition Database Form 042018 4Document11 pagesCole Kelby Nutrition Database Form 042018 4api-381003133100% (1)
- Medical Nutrition Therapy For DiabetesDocument27 pagesMedical Nutrition Therapy For Diabetesdr.Uci BaharNo ratings yet
- Nutritional Guidelines Menu Checklist: For Residential and Nursing HomesDocument54 pagesNutritional Guidelines Menu Checklist: For Residential and Nursing HomesJeffrey PeekoNo ratings yet
- NCPPartIII2019 PDFDocument28 pagesNCPPartIII2019 PDFjothiNo ratings yet
- 8 16 Dietary Analysis ProjectDocument4 pages8 16 Dietary Analysis ProjectMatt HubbsNo ratings yet
- PES StatementsDocument6 pagesPES Statementsdoniazad13112100% (1)
- Boyd Short Presentation SlidesDocument10 pagesBoyd Short Presentation Slidesapi-347518401No ratings yet
- Boyd Coaching and Research GrantDocument3 pagesBoyd Coaching and Research Grantapi-347518401No ratings yet
- Boyd Clinical Case Study 2Document29 pagesBoyd Clinical Case Study 2api-347518401No ratings yet
- Nut 118 Final ProjectDocument4 pagesNut 118 Final Projectapi-347518401No ratings yet
- Biomedical Waste Management PDFDocument8 pagesBiomedical Waste Management PDFSujatha J JayabalNo ratings yet
- Pakistan Medical & Dental Council (PM&DC) - 1Document32 pagesPakistan Medical & Dental Council (PM&DC) - 1Cricket LoverNo ratings yet
- 3075-Article Text-9088-1-10-20201218Document11 pages3075-Article Text-9088-1-10-20201218Rasdawati RasulNo ratings yet
- Slim SpurlingDocument217 pagesSlim SpurlingEli king100% (1)
- 6BDocument28 pages6BLidia Meylin Rivero LoayzaNo ratings yet
- Videsh PrintingDocument22 pagesVidesh PrintingAbroadnayak KumarNo ratings yet
- The Efficacy of Homoeopathic Medicines in Treatment of Amenorrhoea.20200718114308Document9 pagesThe Efficacy of Homoeopathic Medicines in Treatment of Amenorrhoea.20200718114308Azam alausyNo ratings yet
- Types of Cast and Indications: Daisy Jane Antipuesto RN MNDocument3 pagesTypes of Cast and Indications: Daisy Jane Antipuesto RN MNPhylum ChordataNo ratings yet
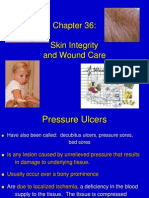
- Skin Integrity and Wound CareDocument55 pagesSkin Integrity and Wound Caremango47No ratings yet
- Antibody Structure and Function: Parham - Chapter 2Document66 pagesAntibody Structure and Function: Parham - Chapter 2Vishnu Reddy Vardhan PulimiNo ratings yet
- Oxygen DeliveryDocument6 pagesOxygen Deliveryyourdirtysocks100% (1)
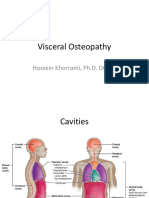
- Visceral Anatomy For OsteopathyDocument152 pagesVisceral Anatomy For OsteopathyHossein Khorrami100% (1)
- Blood Supply of The Brain: by Dr. Noura El TahawyDocument100 pagesBlood Supply of The Brain: by Dr. Noura El TahawySureshNo ratings yet
- Lilyasari2019 Article EconomicEvaluationOfSildenafilDocument9 pagesLilyasari2019 Article EconomicEvaluationOfSildenafilNajib Al FatinNo ratings yet
- Blood ProductDocument89 pagesBlood ProductSam0% (1)
- CDC - DPDX - Intestinal CapillariasisDocument10 pagesCDC - DPDX - Intestinal CapillariasisApril Mae Palomares PunayNo ratings yet
- Acute Ischemic Stroke PathwayDocument50 pagesAcute Ischemic Stroke PathwaydjizhieeNo ratings yet
- UK National Guideline For The Management of Pelvic Inflamatory DiseaseDocument18 pagesUK National Guideline For The Management of Pelvic Inflamatory Diseasealejandro perez sanchezNo ratings yet
- HLSC 3570 ReferencesDocument2 pagesHLSC 3570 Referencesapi-335982597No ratings yet
- Rubidium Myocardial Perfusion ScanDocument2 pagesRubidium Myocardial Perfusion ScanRadlinkSingaporeNo ratings yet
- Drug of ChoiceDocument2 pagesDrug of ChoiceRia Tiglao Fortugaliza100% (1)
- SEXPresentation Woolsey Hall HPDocument86 pagesSEXPresentation Woolsey Hall HPJohnSibmeNo ratings yet
- 5 Amazing Health Benefits & Uses of Athimadhuram Tea/ Mulethi Tea + RecipeDocument21 pages5 Amazing Health Benefits & Uses of Athimadhuram Tea/ Mulethi Tea + RecipeBhuvanesh JayakumarNo ratings yet
- PMLSP 2 ReviewerDocument38 pagesPMLSP 2 ReviewerSophia Mae ClavecillaNo ratings yet
- Arrasn Genreanalysis FinalDocument8 pagesArrasn Genreanalysis Finalapi-294962929No ratings yet
- Encyclopedia of Folk Medicine: Old World and New World TraditionsDocument4 pagesEncyclopedia of Folk Medicine: Old World and New World TraditionsDrflora Eg100% (1)
- Feline Infectious Peritonitis (FIP) - Now A Treatable Disease'Document6 pagesFeline Infectious Peritonitis (FIP) - Now A Treatable Disease'Dr adarsh BijapurNo ratings yet
- Irregular Verbs ListDocument4 pagesIrregular Verbs ListmeddebyounesNo ratings yet
- Maria Deleanu Carte de BucateDocument68 pagesMaria Deleanu Carte de BucateAnonymous 52KH7Ki95No ratings yet
- Modern Professional Business LetterheadDocument2 pagesModern Professional Business LetterheadSalinda TennakoonNo ratings yet