You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
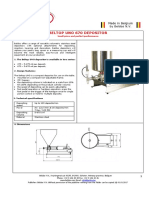
- The Beltop UNO Depositor Is Available in Two SeriesDocument5 pagesThe Beltop UNO Depositor Is Available in Two SeriesJonathan FajardoNo ratings yet
- UAS Bahasa Inggris Kelas IV Semester 1 QuestionsDocument2 pagesUAS Bahasa Inggris Kelas IV Semester 1 QuestionsSetiawan ArifNo ratings yet
- KSK Food Products Overcomes Challenges with Strategic PlanningDocument5 pagesKSK Food Products Overcomes Challenges with Strategic PlanningBonitoNo ratings yet
- HulDocument18 pagesHulGorang MuthaNo ratings yet
- TAX02 Lecture Input TaxDocument5 pagesTAX02 Lecture Input TaxJames DiazNo ratings yet
- Present Simple Tense Reference GuideDocument7 pagesPresent Simple Tense Reference GuideViktoryia KimstachNo ratings yet
- SOP Standard Operating Procedures F&B Service. (Room Service)Document8 pagesSOP Standard Operating Procedures F&B Service. (Room Service)Raden Bambang EkalawiyaNo ratings yet
- English Summer Course For Smarten KidsDocument48 pagesEnglish Summer Course For Smarten KidsSmarten Academy100% (1)
- Iron Deficiency Anaemia: DR Mrs Stella Kanu Bmls Mbbs MSCDocument17 pagesIron Deficiency Anaemia: DR Mrs Stella Kanu Bmls Mbbs MSCDavid KanuNo ratings yet
- Bio320 Lab 2Document4 pagesBio320 Lab 2Mirza KarmilaNo ratings yet
- 6 Week Weight Loss ChallengeDocument6 pages6 Week Weight Loss Challengerunrg100% (25)
- Family Menu ProjectDocument20 pagesFamily Menu ProjectRavenNo ratings yet
- More Than One SecretDocument125 pagesMore Than One SecretSofiaNo ratings yet
- Consolidated Worksheet of Reversible IrreversibleDocument15 pagesConsolidated Worksheet of Reversible IrreversibleAngkita KiranaNo ratings yet
- SWOT PepsiCoDocument4 pagesSWOT PepsiCoKapil NitharwalNo ratings yet
- Ent QuestionaireDocument2 pagesEnt QuestionaireNoman AnsariNo ratings yet
- TLE-6-W8 (Autosaved)Document25 pagesTLE-6-W8 (Autosaved)Khan S AbtahiNo ratings yet
- Action PlanDocument2 pagesAction PlanNadosh HijaziNo ratings yet
- Manufacturing Processes for ForksDocument6 pagesManufacturing Processes for ForksTiNie OuCrewNo ratings yet
- Major Spice Crops in Ethiopia: Production and Export StatusDocument15 pagesMajor Spice Crops in Ethiopia: Production and Export StatusHayyuu Hassen100% (1)
- Authentic Soups and Dishes from AsiaDocument3 pagesAuthentic Soups and Dishes from AsiaShafiqul ChowdhuryNo ratings yet
- Preschool Materials Guide: Herman T. Knopf & Kerrie L. WelshDocument50 pagesPreschool Materials Guide: Herman T. Knopf & Kerrie L. Welshjade tagabNo ratings yet
- Home Budget CalculatorDocument4 pagesHome Budget CalculatoraliasgarNo ratings yet
- The Cooking Oil and Ghee Industry Was Heavily Burdened With TaxesDocument2 pagesThe Cooking Oil and Ghee Industry Was Heavily Burdened With TaxesfahimfayazfahimfayazNo ratings yet
- Casa De Soya's Business EnvironmentDocument4 pagesCasa De Soya's Business EnvironmentMacy LacabaNo ratings yet
- Handbook of Trail Campcraft 1954Document196 pagesHandbook of Trail Campcraft 1954shivadogNo ratings yet
- ITC Report and Accounts 2019 PDFDocument344 pagesITC Report and Accounts 2019 PDFMegha GoyalNo ratings yet
- Odyssey Book 13Document24 pagesOdyssey Book 13Jenna ParkerNo ratings yet
- STD Ii Package No 2 1Document186 pagesSTD Ii Package No 2 1Trump Donald100% (1)
- Host Script 1Document5 pagesHost Script 1jerson hidalgoNo ratings yet