You might also like
- Eye ManualDocument56 pagesEye Manualbashir019No ratings yet
- Water Colored Splashes PowerPoint TemplateDocument36 pagesWater Colored Splashes PowerPoint TemplateAna Carmela DomingoNo ratings yet
- The Open Ophthalmology JournalDocument5 pagesThe Open Ophthalmology JournalFenny Duma SariNo ratings yet
- Abstrack Delibrate PracticeDocument2 pagesAbstrack Delibrate PracticetopNo ratings yet
- Slit LampbiomicrosDocument18 pagesSlit LampbiomicrostopNo ratings yet
- Kertas Resep YudiDocument1 pageKertas Resep YuditopNo ratings yet
- Pediatric Non-Hodgkin Lymphoma Differential DiagnosesDocument2 pagesPediatric Non-Hodgkin Lymphoma Differential DiagnosestopNo ratings yet
- Pediatric Non-Hodgkin Lymphoma - Background, Etiology, EpidemiologyDocument11 pagesPediatric Non-Hodgkin Lymphoma - Background, Etiology, EpidemiologytopNo ratings yet
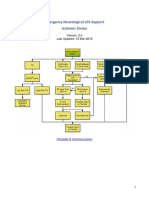
- Emergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Document22 pagesEmergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Aik NoeraNo ratings yet
- Pediatric Non-Hodgkin Lymphoma Treatment & Management: Approach ConsiderationsDocument15 pagesPediatric Non-Hodgkin Lymphoma Treatment & Management: Approach ConsiderationstopNo ratings yet
- Pediatric Non-Hodgkin Lymphoma Workup - Approach Considerations, Laboratory Studies, Imaging StudiesDocument5 pagesPediatric Non-Hodgkin Lymphoma Workup - Approach Considerations, Laboratory Studies, Imaging StudiestopNo ratings yet
- Felting Fabulous Flowers Templates PDFDocument3 pagesFelting Fabulous Flowers Templates PDFtop67% (3)
- Eye TraumaDocument19 pagesEye TraumatopNo ratings yet
- Pediatric Non-Hodgkin Lymphoma MedicationDocument8 pagesPediatric Non-Hodgkin Lymphoma MedicationtopNo ratings yet
- Total ModalDocument1 pageTotal ModaltopNo ratings yet
- Role of PET/CT in Malignant Pediatric Lymphoma: Original ArticleDocument11 pagesRole of PET/CT in Malignant Pediatric Lymphoma: Original ArticletopNo ratings yet
- Pediatric Non-Hodgkin Lymphoma Clinical Presentation - History, Physical ExaminationDocument3 pagesPediatric Non-Hodgkin Lymphoma Clinical Presentation - History, Physical ExaminationtopNo ratings yet
- CSS Jurnal DR IdratDocument8 pagesCSS Jurnal DR IdrattopNo ratings yet
- Jurnal Asli CSS - Khalida Khairunnisa - DR - ErniDocument7 pagesJurnal Asli CSS - Khalida Khairunnisa - DR - ErnitopNo ratings yet
- Role of Limited Whole-BodyDocument9 pagesRole of Limited Whole-BodytopNo ratings yet
- Poster Publik & Poster IlmiahDocument10 pagesPoster Publik & Poster Ilmiahtop100% (1)
- Materi Lat DesignDocument27 pagesMateri Lat DesigntopNo ratings yet
- Presentation 1Document8 pagesPresentation 1topNo ratings yet
- Radiologic Clinics of North America Volume 46 Issue 2 2008 (Doi 10.1016/j.rcl.2008.03.009) Abramson, Sara J. Price, Anita P. - Imaging of Pediatric LymphomasDocument26 pagesRadiologic Clinics of North America Volume 46 Issue 2 2008 (Doi 10.1016/j.rcl.2008.03.009) Abramson, Sara J. Price, Anita P. - Imaging of Pediatric LymphomastopNo ratings yet
- NSI in Pediatric Rhinosinusitis PDFDocument19 pagesNSI in Pediatric Rhinosinusitis PDFtopNo ratings yet
- Guideline AoeDocument25 pagesGuideline AoetopNo ratings yet
- Antihistamines For Treating RhinosinusitisDocument6 pagesAntihistamines For Treating RhinosinusitistopNo ratings yet
- Role of Isotonic Saline Nasal Irrigation in Seasonal Allergic RhinitisDocument5 pagesRole of Isotonic Saline Nasal Irrigation in Seasonal Allergic RhinitistopNo ratings yet
- Antibiotics in Chronic RhinosinusitisDocument5 pagesAntibiotics in Chronic RhinosinusitistopNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Physiology of ItchingDocument25 pagesPhysiology of ItchingElGreco03No ratings yet
- A&P Review Questions-1Document20 pagesA&P Review Questions-1phillip_galinsyNo ratings yet
- Lecture 9. Physiology of Autonomic Nervous SystemDocument19 pagesLecture 9. Physiology of Autonomic Nervous SystemJaime Japana III100% (2)
- INTROPSY Reviewer (Book and Lecture Notes) Chapters 1 and 2Document11 pagesINTROPSY Reviewer (Book and Lecture Notes) Chapters 1 and 2jonaxx enthusiastNo ratings yet
- Nicotine - WikipediaDocument30 pagesNicotine - WikipediaHeaven2012No ratings yet
- POLYGRAPHYDocument7 pagesPOLYGRAPHYAries Gallandez100% (2)
- Dwnload Full Invitation To Psychology 7th Edition Wade Test Bank PDFDocument35 pagesDwnload Full Invitation To Psychology 7th Edition Wade Test Bank PDFezracook12mo100% (11)
- Measureable Changes in The Neuro-Endocrinal Mechanism Following Spinal Manipulation - 2015Document6 pagesMeasureable Changes in The Neuro-Endocrinal Mechanism Following Spinal Manipulation - 2015Renan O. Pravatta PivettaNo ratings yet
- Astro Diagnosis Libra Part ADocument26 pagesAstro Diagnosis Libra Part AOvn MurthyNo ratings yet
- The Somatic Nervous System The Autonomic Nervous System - The Enteric Nervous SystemDocument5 pagesThe Somatic Nervous System The Autonomic Nervous System - The Enteric Nervous SystemMarissa AsimNo ratings yet
- Neuron System QuestionDocument15 pagesNeuron System QuestionShela Huang100% (1)
- Cardiovascular NotesDocument23 pagesCardiovascular NotesEmily DongNo ratings yet
- Nervous System 4 PDF FreeDocument15 pagesNervous System 4 PDF FreeZedy GullesNo ratings yet
- Local Anesthesia in DentistryDocument260 pagesLocal Anesthesia in DentistryKishendran R GanandranNo ratings yet
- Psychology 114 Completed PDFDocument80 pagesPsychology 114 Completed PDFGrace AndersonNo ratings yet
- Psychology 4th Edition Schacter Test BankDocument86 pagesPsychology 4th Edition Schacter Test BankdawnholmesrtcongdbszNo ratings yet
- 04 - 36-40 - Visceral Motor System - Functional Anatomical DivisionsDocument5 pages04 - 36-40 - Visceral Motor System - Functional Anatomical DivisionsPedja LeyNo ratings yet
- Book Janig PDFDocument634 pagesBook Janig PDFMarcus Dos SantosNo ratings yet
- Unit 2 Medicinal Chemistry 4th Semester McqsDocument52 pagesUnit 2 Medicinal Chemistry 4th Semester Mcqschannel jollyhood100% (2)
- NCM 106 (PHARMA) - Lec 19 To 28Document18 pagesNCM 106 (PHARMA) - Lec 19 To 28Aine Jermaine GatchalianNo ratings yet
- Breathwork Basics EbookDocument11 pagesBreathwork Basics EbookBakulBadwalNo ratings yet
- BIO130 Chapter 15&16 SlidesDocument26 pagesBIO130 Chapter 15&16 SlidesTheophilus BaidooNo ratings yet
- Ch. 2 Critical Thinking ActivityDocument7 pagesCh. 2 Critical Thinking ActivityYe Yusi100% (1)
- Spinal Cord InjuryDocument37 pagesSpinal Cord InjuryMrmonstrosityNo ratings yet
- General Pharmacology NotesDocument67 pagesGeneral Pharmacology NotesZehra KhanNo ratings yet
- Polygraph ReviewerDocument13 pagesPolygraph ReviewerVito Don83% (18)
- Introduction To Digestive System: Creat by Vedant PatelDocument21 pagesIntroduction To Digestive System: Creat by Vedant PatelVedant PatelNo ratings yet
- Breathing To Treat Vagus NerveDocument13 pagesBreathing To Treat Vagus NerveImad Mukahhal100% (7)
- Journal Reading Marsya Y Loppies 201283003Document16 pagesJournal Reading Marsya Y Loppies 201283003Marsya Yulinesia LoppiesNo ratings yet
- Abnormal Psychology Notes Barlow & Durand, "Abnormal Psychology" Black & Grant "DSM V Guidebook"Document54 pagesAbnormal Psychology Notes Barlow & Durand, "Abnormal Psychology" Black & Grant "DSM V Guidebook"Kat Torralba100% (1)