You might also like
- Unhealthy Food Consumption in Adolescence: Role of Sedentary Behaviours and Modifiers in 11-, 13-And 15-Year-Old ItaliansDocument7 pagesUnhealthy Food Consumption in Adolescence: Role of Sedentary Behaviours and Modifiers in 11-, 13-And 15-Year-Old ItaliansJason DenostaNo ratings yet
- Associations Between Soft-Drink ConsumptionDocument9 pagesAssociations Between Soft-Drink ConsumptionkarinaNo ratings yet
- Adlosent Nutrition DelisleDocument38 pagesAdlosent Nutrition DelisleAnonymous QLxHwZ0LTKNo ratings yet
- Fast FoodDocument8 pagesFast Foodkangna_sharma20No ratings yet
- Food environments of young people linked to dietDocument10 pagesFood environments of young people linked to dietefrandusNo ratings yet
- Nurturing a Healthy Generation of Children: Research Gaps and Opportunities: 91st Nestlé Nutrition Institute Workshop, Manila, March 2018From EverandNurturing a Healthy Generation of Children: Research Gaps and Opportunities: 91st Nestlé Nutrition Institute Workshop, Manila, March 2018No ratings yet
- Nutrients 10 00559 v2 PDFDocument12 pagesNutrients 10 00559 v2 PDFJaveria WaheedNo ratings yet
- Nutrients: Dietary Behavior and Physical Activity in Children and AdolescentsDocument4 pagesNutrients: Dietary Behavior and Physical Activity in Children and AdolescentsmiraandrianiNo ratings yet
- Chapte 1 2 - Group 5 1Document19 pagesChapte 1 2 - Group 5 1arlenetacla12No ratings yet
- Older Adults and Patients in Need of Nutritional Support Review of CurrentDocument10 pagesOlder Adults and Patients in Need of Nutritional Support Review of CurrentimwinnerNo ratings yet
- The Road To Good NutritionDocument221 pagesThe Road To Good NutritionSenyum SehatNo ratings yet
- Impact of early life nutrition on health outcomesDocument28 pagesImpact of early life nutrition on health outcomesAgung GuretnoNo ratings yet
- A. Ruíz-Roso Et Al 2020 - Changes of Physical Activity and Ultraprocessed Food Consumption in Adolescents From Different Countries During Covid19Document13 pagesA. Ruíz-Roso Et Al 2020 - Changes of Physical Activity and Ultraprocessed Food Consumption in Adolescents From Different Countries During Covid19Natale FigueiredoNo ratings yet
- HLGuide22 23Document38 pagesHLGuide22 23Luis Gerardo Aguilar CruzNo ratings yet
- Aging & ApetiteDocument114 pagesAging & ApetiteStefanie DitaNo ratings yet
- Artículo de La EpidemiologiaDocument3 pagesArtículo de La EpidemiologiaPaulaNo ratings yet
- Policies To Prevent Childhood Obesity in The European Union: T. Lobstein, L. A. BaurDocument4 pagesPolicies To Prevent Childhood Obesity in The European Union: T. Lobstein, L. A. BaurruxandraplNo ratings yet
- Sustainable Diets: Linking Nutrition and Food SystemsFrom EverandSustainable Diets: Linking Nutrition and Food SystemsBarbara BurlingameNo ratings yet
- Am J Clin Nutr 2012 Verstraeten 415 38Document24 pagesAm J Clin Nutr 2012 Verstraeten 415 38JelnathleeNo ratings yet
- Craveiro Et Al. 2021 ApettiteDocument10 pagesCraveiro Et Al. 2021 ApettiteSilvestre Garcia de JalonNo ratings yet
- Nutritional Epidemiology-Past, Present, Future: EditorialDocument3 pagesNutritional Epidemiology-Past, Present, Future: Editorialisabel sedanoNo ratings yet
- Are School Meals A Viable and Sustainable Tool To Improve The Healthiness and Sustainability of Children S Diet and Food Consumption A Cross NationalDocument18 pagesAre School Meals A Viable and Sustainable Tool To Improve The Healthiness and Sustainability of Children S Diet and Food Consumption A Cross NationalAndreia BorgesNo ratings yet
- Nutrients 10 01439 v3 PDFDocument23 pagesNutrients 10 01439 v3 PDFmNo ratings yet
- (Adam Drenowski) Obesity Treatment and Prevention New DirectionsDocument166 pages(Adam Drenowski) Obesity Treatment and Prevention New DirectionsAlexandraNo ratings yet
- Assignment 2 Hasan - Muhammad TarequeDocument4 pagesAssignment 2 Hasan - Muhammad TarequeRozen TarequeNo ratings yet
- Community Nutrition Nestle Nutrition InstituteDocument4 pagesCommunity Nutrition Nestle Nutrition InstituteOsamaNo ratings yet
- WHO NutritionDocument108 pagesWHO NutritionJanka CoronelNo ratings yet
- Strategies and Interventions For Healthy Adolescent Growth, Nutrition, and DevelopmentDocument13 pagesStrategies and Interventions For Healthy Adolescent Growth, Nutrition, and DevelopmentsilviaNo ratings yet
- Identification of Several EatiDocument11 pagesIdentification of Several EatiNs. Dini Tryastuti, M.Kep.,Sp.Kep.,KomNo ratings yet
- Vegetarian Diets in Children: A Systematic Review: S. Schürmann M. Kersting U. AlexyDocument21 pagesVegetarian Diets in Children: A Systematic Review: S. Schürmann M. Kersting U. Alexynehorai harbiNo ratings yet
- Food Neophobia Is Related To Factors Associated With Functional Food Consumption in Older AdultsDocument8 pagesFood Neophobia Is Related To Factors Associated With Functional Food Consumption in Older AdultsrodrigoromoNo ratings yet
- Out-Of-Home Eating Frequency, Causal Attribution of Obesity and Support To Healthy Eating Policies From A Cross-European SurveyDocument13 pagesOut-Of-Home Eating Frequency, Causal Attribution of Obesity and Support To Healthy Eating Policies From A Cross-European SurveyBio BaniNo ratings yet
- Clinical Nutrition and Human Rights An International Po 2021 Clinical NutriDocument8 pagesClinical Nutrition and Human Rights An International Po 2021 Clinical NutriArie Dwi ANo ratings yet
- Enteral Nutrition in Dementia A Systematic ReviewDocument13 pagesEnteral Nutrition in Dementia A Systematic ReviewAkim DanielNo ratings yet
- Adolescent Nutrition PaperDocument38 pagesAdolescent Nutrition PaperArief Budiman50% (2)
- Eat Right, Live Well Understanding the Science of NutritionFrom EverandEat Right, Live Well Understanding the Science of NutritionNo ratings yet
- Nutritional Status of Grade Pupils of San Roque Elementary School San Jacinto, PangasinanDocument39 pagesNutritional Status of Grade Pupils of San Roque Elementary School San Jacinto, PangasinanmharicharNo ratings yet
- Satish C. Kalhan, Andrew M. Prentice, Chittaranjan S. Yajnik - Emerging Societies - Coexistence of Childhood Malnutrition and Obesity (Nestle Nutrition Workshop Series_ Pediatric Program)-S. Karger AG.pdfDocument281 pagesSatish C. Kalhan, Andrew M. Prentice, Chittaranjan S. Yajnik - Emerging Societies - Coexistence of Childhood Malnutrition and Obesity (Nestle Nutrition Workshop Series_ Pediatric Program)-S. Karger AG.pdfBelmar Steven Papamija OrtizNo ratings yet
- Family Nutrition GuideFrom EverandFamily Nutrition GuideNo ratings yet
- New AssignmentDocument3 pagesNew AssignmentDrew JoanNo ratings yet
- Viewpoint Article: Childhood Obesity - Looking Back Over 50 Years To Begin To Look ForwardDocument5 pagesViewpoint Article: Childhood Obesity - Looking Back Over 50 Years To Begin To Look ForwardichalsajaNo ratings yet
- Understanding the Lived Experiences of Obese High School StudentsDocument7 pagesUnderstanding the Lived Experiences of Obese High School StudentsMichael Charles James GingcoNo ratings yet
- EJCM - Volume 36 - Issue 1 - Pages 45-60-1Document16 pagesEJCM - Volume 36 - Issue 1 - Pages 45-60-1Yaumil FauziahNo ratings yet
- Why Study Global Health?: Amatya A, Basel PDocument2 pagesWhy Study Global Health?: Amatya A, Basel PRika AskiaNo ratings yet
- Research Paper On Childhood Obesity in IndiaDocument7 pagesResearch Paper On Childhood Obesity in Indiafvg1rph4100% (1)
- Assignment TemplateDocument9 pagesAssignment TemplateAbcd 1234No ratings yet
- DessieDocument10 pagesDessieLemma BerisoNo ratings yet
- Mini Nutritional AssessmentDocument7 pagesMini Nutritional AssessmentJoão Mariano SantosNo ratings yet
- Literature Review On Causes of Childhood ObesityDocument4 pagesLiterature Review On Causes of Childhood Obesityjsmyxkvkg100% (1)
- Nutrients: Nutritional Habits and Interventions in ChildhoodDocument5 pagesNutrients: Nutritional Habits and Interventions in ChildhoodBBD BBDNo ratings yet
- Nutrients: Factors Influencing Dietary Patterns During Pregnancy in A Culturally Diverse SocietyDocument20 pagesNutrients: Factors Influencing Dietary Patterns During Pregnancy in A Culturally Diverse SocietyAngelika DomondonNo ratings yet
- Articless41572 023 00435 4.Pdfpdf Button20stickyDocument19 pagesArticless41572 023 00435 4.Pdfpdf Button20stickyTabitha MenezesNo ratings yet
- Running Head: Unit 9 Assignment-Nutrition Education Guide 1Document26 pagesRunning Head: Unit 9 Assignment-Nutrition Education Guide 1api-398844359No ratings yet
- Nutrition Chapter 1Document6 pagesNutrition Chapter 1Eliani BrianNo ratings yet
- Nutrition Support For Infants and Children at Risk PDFDocument253 pagesNutrition Support For Infants and Children at Risk PDFarmanto100% (1)
- Assessment of Nutritional Knowledge, Food Consumption and Personal Hygiene of AdolescentsDocument6 pagesAssessment of Nutritional Knowledge, Food Consumption and Personal Hygiene of AdolescentsTJPRC PublicationsNo ratings yet
- Poor Nutrition ProjectDocument60 pagesPoor Nutrition Projectaniamulu munachimNo ratings yet
- Practical Applications: A New Index Proposed For Determination of Outcome of Recession Coverage ProceduresDocument7 pagesPractical Applications: A New Index Proposed For Determination of Outcome of Recession Coverage ProceduresCristian OneaNo ratings yet
- Oral Hygiene Habits of 11-Year-Olds in 23 CountriesDocument8 pagesOral Hygiene Habits of 11-Year-Olds in 23 CountriesCristian OneaNo ratings yet
- Trimming HoDocument6 pagesTrimming HoCristian OneaNo ratings yet
- Variation in Cuspal Morphology in Maxillary First Permanent Molar With Report of 3 Cusp Molar-A Prevalence StudyDocument3 pagesVariation in Cuspal Morphology in Maxillary First Permanent Molar With Report of 3 Cusp Molar-A Prevalence StudyCristian OneaNo ratings yet
- Case Series: The Use of Enamel Matrix Derivative in Two-Stage Guided Bone Regeneration ProceduresDocument8 pagesCase Series: The Use of Enamel Matrix Derivative in Two-Stage Guided Bone Regeneration ProceduresCristian OneaNo ratings yet
- Art 2Document6 pagesArt 2Cristian OneaNo ratings yet
- Dentofacial Orthopeadics in Pediatric DentistryDocument4 pagesDentofacial Orthopeadics in Pediatric DentistryCristian OneaNo ratings yet
- Practical ApplicationsDocument9 pagesPractical ApplicationsCristian OneaNo ratings yet
- REGENERATING FURCATIONSDocument10 pagesREGENERATING FURCATIONSCristian OneaNo ratings yet
- Does Timing of Eruption in First Primary Tooth Correlate With That of First Permanent Tooth? A 9-Year Cohort StudyDocument7 pagesDoes Timing of Eruption in First Primary Tooth Correlate With That of First Permanent Tooth? A 9-Year Cohort StudyCristian OneaNo ratings yet
- Relationship Between Dental Size and Normal Occlusion in Brazilian PatientsDocument5 pagesRelationship Between Dental Size and Normal Occlusion in Brazilian PatientsCristian OneaNo ratings yet
- Proper Model Trimming Technique for Orthodontic DiagnosisDocument4 pagesProper Model Trimming Technique for Orthodontic DiagnosisRajesh Gyawali100% (1)
- Aging and PeriodontiumDocument5 pagesAging and PeriodontiumCristian OneaNo ratings yet
- Dental Erosive Wear and Salivary Flow RateDocument8 pagesDental Erosive Wear and Salivary Flow RateCristian OneaNo ratings yet
- The Relationship Between Irregularity of The Incisor Teeth, Plaque, and Gingivitis: A Study in A Group of Schoolchildren Aged 11-14 YearsDocument8 pagesThe Relationship Between Irregularity of The Incisor Teeth, Plaque, and Gingivitis: A Study in A Group of Schoolchildren Aged 11-14 YearsCristian OneaNo ratings yet
- LittleDocument5 pagesLittleCristian OneaNo ratings yet
- An Approach To Maintain Orthodontic Alignment of Lower Incisors Without The Use of RetainersDocument6 pagesAn Approach To Maintain Orthodontic Alignment of Lower Incisors Without The Use of RetainersCristian OneaNo ratings yet
- Assessment of Supracrestal Gingival TissueDocument2 pagesAssessment of Supracrestal Gingival TissueCristian OneaNo ratings yet
- Correlation in Mandibular Length and Third Molar MaturationDocument7 pagesCorrelation in Mandibular Length and Third Molar MaturationCristian OneaNo ratings yet
- A Simultaneous Mobilization of Four Impacted Upper Incisors in A Case of An Adolescent Patient With Cleidocranial Dysplasia CCD 2161 1122.1000210Document8 pagesA Simultaneous Mobilization of Four Impacted Upper Incisors in A Case of An Adolescent Patient With Cleidocranial Dysplasia CCD 2161 1122.1000210Cristian OneaNo ratings yet
- A Content Analysis of Children's Television Advertising: Focus On Food and Oral HealthDocument8 pagesA Content Analysis of Children's Television Advertising: Focus On Food and Oral HealthCristian OneaNo ratings yet
- Gender Differences For Deciduous Molar Sizes in Children of Jammu CityDocument3 pagesGender Differences For Deciduous Molar Sizes in Children of Jammu CityCristian OneaNo ratings yet
- Effect On Caries of Restricting Sugars IntakeDocument11 pagesEffect On Caries of Restricting Sugars IntakeCristian OneaNo ratings yet
- Sugar and Health: A Food-Based Dietary Guideline For South AfricaDocument5 pagesSugar and Health: A Food-Based Dietary Guideline For South AfricaCristian OneaNo ratings yet
- Interrelationship Between Diet and Oral HealthDocument10 pagesInterrelationship Between Diet and Oral HealthCristian OneaNo ratings yet
- Caries and Quality of Life in Portuguese Adolescents: Impact of Diet and Behavioural Risk FactorsDocument6 pagesCaries and Quality of Life in Portuguese Adolescents: Impact of Diet and Behavioural Risk FactorsCristian OneaNo ratings yet
- Access To Excess: How Do Adolescents Deal With Unhealthy Foods in Their Environment?Document5 pagesAccess To Excess: How Do Adolescents Deal With Unhealthy Foods in Their Environment?Cristian OneaNo ratings yet
- The ContributionDocument5 pagesThe ContributionCristian OneaNo ratings yet
- Effectsofsoftdrinksondentalhealth AreviewDocument11 pagesEffectsofsoftdrinksondentalhealth AreviewCristian OneaNo ratings yet
- OMS 2005 Nutritia Si Patologia Orala PDFDocument6 pagesOMS 2005 Nutritia Si Patologia Orala PDFSabina IoanaNo ratings yet
- The Induction ProcessDocument5 pagesThe Induction ProcessP Kranthi KiranNo ratings yet
- PoetryDocument22 pagesPoetryYakini GazaEmpress HowellNo ratings yet
- Moonshining Guide PDFDocument7 pagesMoonshining Guide PDFanunessnNo ratings yet
- Aavin Summer Internship ReportDocument45 pagesAavin Summer Internship Reportmo25% (4)
- Abdulqader Et Al 2000 Spirulina Harvesting ChadDocument6 pagesAbdulqader Et Al 2000 Spirulina Harvesting ChadDan H KeremNo ratings yet
- Slyman S Restaurant MenuDocument3 pagesSlyman S Restaurant MenueatlocalmenusNo ratings yet
- Teachers Book Tronsmall NICO'sDocument205 pagesTeachers Book Tronsmall NICO'sCarolina Cautivo100% (1)
- WorldofeastereggsDocument7 pagesWorldofeastereggsapi-265783879No ratings yet
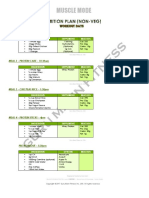
- MuscleMode NutritionPlan by Guru MannDocument6 pagesMuscleMode NutritionPlan by Guru MannTilak RajNo ratings yet
- Recipe BookDocument35 pagesRecipe BookYana WatanabeNo ratings yet
- City Pages January 2010 Volume 1Document76 pagesCity Pages January 2010 Volume 1febbinsNo ratings yet
- Metro Wine Center: All The Wines and Liquor You NeedDocument2 pagesMetro Wine Center: All The Wines and Liquor You NeedCarmela CalangiNo ratings yet
- Strategic Analysis Of StarbucksDocument17 pagesStrategic Analysis Of StarbucksJasweetSinghNo ratings yet
- Food-Safety Zone-Restaurant-List PDFDocument4 pagesFood-Safety Zone-Restaurant-List PDFNasser FaridNo ratings yet
- Neighbors MenuDocument2 pagesNeighbors MenuMatt BennettNo ratings yet
- Worksheet EnglishDocument8 pagesWorksheet EnglishFlor MallquiNo ratings yet
- Revised Assignment OneDocument9 pagesRevised Assignment OneMorgan BittleNo ratings yet
- Petes Fish and ChipsDocument1 pagePetes Fish and Chipsapi-307746974No ratings yet
- Whiteswaen©Dark: Parameter Unit Min Max UsageDocument1 pageWhiteswaen©Dark: Parameter Unit Min Max UsageVivi LealNo ratings yet
- Malay Culture Project - Malay Food & Etiquette (Autosaved)Document11 pagesMalay Culture Project - Malay Food & Etiquette (Autosaved)Soap MacTavish100% (1)
- Juan Luna's Dark SideDocument28 pagesJuan Luna's Dark SideJannel Balunsat BasiuangNo ratings yet
- Bamboo Nutritional AnalysisDocument3 pagesBamboo Nutritional AnalysisAmanda BrunerNo ratings yet
- Sugar, Enriched Flour (Wheat Flour, Niacin, Reduced Iron, Thiamine Mononitrate (Vitamin B1), Riboflavin (Vitamin B2), FolicDocument2 pagesSugar, Enriched Flour (Wheat Flour, Niacin, Reduced Iron, Thiamine Mononitrate (Vitamin B1), Riboflavin (Vitamin B2), FolicSkater KoiNo ratings yet
- English Listening Test ReviewDocument20 pagesEnglish Listening Test ReviewSufiandi CarolineNo ratings yet
- A Recipe Book of Traditional Sri Lankan FoodDocument5 pagesA Recipe Book of Traditional Sri Lankan FoodRushan LakdimuthuNo ratings yet
- Damiana Turnera Diffusa Materia Medica HerbsDocument10 pagesDamiana Turnera Diffusa Materia Medica HerbsAlejandra Guerrero100% (4)
- Plataran Menteng Colonial Mansion Floor Plans and AreasDocument3 pagesPlataran Menteng Colonial Mansion Floor Plans and AreasEshany AshilaNo ratings yet
- Employee Job Satisfaction Study at Mokshwa Soft DrinksDocument76 pagesEmployee Job Satisfaction Study at Mokshwa Soft DrinksAsmina Asmi100% (1)
- Science 3 Q1 - Module 2#Document73 pagesScience 3 Q1 - Module 2#rabalos85No ratings yet
- Evidencia 6 - Segmentation "Describing Potential Clients"Document5 pagesEvidencia 6 - Segmentation "Describing Potential Clients"Brayan andresNo ratings yet