You might also like
- OITE Review 2013Document263 pagesOITE Review 2013addison wood100% (2)
- Nonoperative Treatment of The Medial Malleolus in Bimalleolar and Trimalleolar Ankle Fractures, A Randomized Controlled TrialDocument5 pagesNonoperative Treatment of The Medial Malleolus in Bimalleolar and Trimalleolar Ankle Fractures, A Randomized Controlled TrialDiego Cruces OrdoñezNo ratings yet
- FandAC - 2017 - Hamid - Chronic Rupture of Peroneal TendonsDocument8 pagesFandAC - 2017 - Hamid - Chronic Rupture of Peroneal TendonsJacob DoughertyNo ratings yet
- Joshis External Stabilisation System Jess For Recurrent Ctev Due To Irregular Follow Up PDFDocument5 pagesJoshis External Stabilisation System Jess For Recurrent Ctev Due To Irregular Follow Up PDFshankarNo ratings yet
- Calcanectomy For OsteomyelitisDocument7 pagesCalcanectomy For OsteomyelitisCleff FlowersNo ratings yet
- DF W ReconDocument11 pagesDF W ReconPraveen RavishankaranNo ratings yet
- CHAPTER 14 - Treatment of Bone Def - 2008 - Surgical Techniques of The ShoulderDocument11 pagesCHAPTER 14 - Treatment of Bone Def - 2008 - Surgical Techniques of The ShoulderJaime Vázquez ZárateNo ratings yet
- Complications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFDocument19 pagesComplications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFSergio Tomas Cortés MoralesNo ratings yet
- Wurgaft R, Rappoport K, Soler C, Ponce C, Flores-Mir CDocument16 pagesWurgaft R, Rappoport K, Soler C, Ponce C, Flores-Mir CCatalina Soler LioiNo ratings yet
- Allograft Medial Patellofemoral LigamentDocument11 pagesAllograft Medial Patellofemoral Ligamenttyoinfantil.hegcNo ratings yet
- BF 00265742Document3 pagesBF 00265742angelluis1980No ratings yet
- Physeal Sparing Reconstruction of The Anterior Cruciate Ligament in Skeletally Immature Prepubescent Children and AdolescentsDocument10 pagesPhyseal Sparing Reconstruction of The Anterior Cruciate Ligament in Skeletally Immature Prepubescent Children and AdolescentsPrabhjeet singhNo ratings yet
- Triple Artrodesis TobilloDocument17 pagesTriple Artrodesis TobilloIsrael CucsNo ratings yet
- Medicine The American Journal of SportsDocument8 pagesMedicine The American Journal of Sportshieuminhduong7No ratings yet
- Plantar: Fascia Release For Chronic FasciitisDocument5 pagesPlantar: Fascia Release For Chronic FasciitisAriene RibeiroNo ratings yet
- Pedicle Screw Fixation in Fracture of Thoraco-Lumbar SpineDocument21 pagesPedicle Screw Fixation in Fracture of Thoraco-Lumbar SpineNiyati SharmaNo ratings yet
- MontotenniselbowDocument7 pagesMontotenniselbowPURVA THAKURNo ratings yet
- Use of Allograft in Skeletally Immature Patients For Calcaneal Neck Lengthening OsteotomyDocument5 pagesUse of Allograft in Skeletally Immature Patients For Calcaneal Neck Lengthening OsteotomyMonem ShakeerNo ratings yet
- Latissimus Dorsi Tendon Transfer For Massive, Irreparable Posterosuperior Rotator Cuff Tears: Surgical TechniqueDocument6 pagesLatissimus Dorsi Tendon Transfer For Massive, Irreparable Posterosuperior Rotator Cuff Tears: Surgical TechniquemichellmariottiNo ratings yet
- 10 1097@jsa 0000000000000274Document4 pages10 1097@jsa 0000000000000274Subarna PaudelNo ratings yet
- Pinzamiento de Cadea Pincer CamDocument9 pagesPinzamiento de Cadea Pincer Camvlc driveNo ratings yet
- Effects On Inadvertent Endplate Fracture Following Lateral Cage Placement On Range of Motion and Indirect Spine Decompression in Lumbar Spine Fusion Constructs: A Cadaveric StudyDocument8 pagesEffects On Inadvertent Endplate Fracture Following Lateral Cage Placement On Range of Motion and Indirect Spine Decompression in Lumbar Spine Fusion Constructs: A Cadaveric Studysiti hanifahNo ratings yet
- Rehabilitation and Return To Play Following Meniscal Repair PDFDocument14 pagesRehabilitation and Return To Play Following Meniscal Repair PDFYency AvilaNo ratings yet
- Ankle Stabilization With Arthroscopic Versus Open With Suture Tape Augmentation Techniques X1D XJ. George DeVries PDFDocument5 pagesAnkle Stabilization With Arthroscopic Versus Open With Suture Tape Augmentation Techniques X1D XJ. George DeVries PDFcrpcsxfdkgNo ratings yet
- Nonoperative TreatmentDocument6 pagesNonoperative TreatmentGorkaBuesaNo ratings yet
- Aldrirdge - SurgicalTechDocument16 pagesAldrirdge - SurgicalTechÇağdaş PamukNo ratings yet
- Koreksi KontrakturDocument14 pagesKoreksi KontrakturarifNo ratings yet
- Fronto-Orbital Advancement Using An en Bloc Frontal Bone CraniectomyDocument7 pagesFronto-Orbital Advancement Using An en Bloc Frontal Bone Craniectomyandredwijaya8No ratings yet
- Lateral Tendon Disorders Peroneal Tendinopathy Differential DiagnosisDocument5 pagesLateral Tendon Disorders Peroneal Tendinopathy Differential Diagnosischu_chiang_3No ratings yet
- Daigeler 2009Document8 pagesDaigeler 2009Javier JonesNo ratings yet
- Laprade 2012Document11 pagesLaprade 2012Aaron BNo ratings yet
- MPFL ReconstructionDocument16 pagesMPFL ReconstructiondrjorgewtorresNo ratings yet
- Functional Results After Surgical Treatment For Congenital Knee DislocationDocument8 pagesFunctional Results After Surgical Treatment For Congenital Knee DislocationsarnaoushNo ratings yet
- SHOULDER INSTABILITY ManagDocument18 pagesSHOULDER INSTABILITY ManagFarhan JustisiaNo ratings yet
- Factors Contributing To Relapse in Rigidly Fixed Mandibular SetbacksDocument6 pagesFactors Contributing To Relapse in Rigidly Fixed Mandibular Setbacksabhishekjha0082No ratings yet
- Our Experience On Peroneus Longus As Graft For Arthroscopic ACL ReconstructionDocument9 pagesOur Experience On Peroneus Longus As Graft For Arthroscopic ACL ReconstructionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Meniscal Root Repair Using A Two-Tunnel Technique: Smith&nephewDocument16 pagesMeniscal Root Repair Using A Two-Tunnel Technique: Smith&nephewAlejandro RodriguezNo ratings yet
- Gradual Correction of Knee Flexion Contracture Using External FixationDocument6 pagesGradual Correction of Knee Flexion Contracture Using External Fixationeka aningNo ratings yet
- Instability Procedure: of Ankle and TreatedDocument3 pagesInstability Procedure: of Ankle and TreatedKrishna CaitanyaNo ratings yet
- HTTPS://WWW Mendeley Com/reference-Manager/readerDocument6 pagesHTTPS://WWW Mendeley Com/reference-Manager/readerIJAR JOURNALNo ratings yet
- Develop Med Child Neuro - 2009 - ROOT - Surgical Treatment For Hip Pain in The Adult Cerebral Palsy PatientDocument8 pagesDevelop Med Child Neuro - 2009 - ROOT - Surgical Treatment For Hip Pain in The Adult Cerebral Palsy PatientSitthikorn StrikerrNo ratings yet
- Chalmers 2019Document6 pagesChalmers 2019Spoti PremiNo ratings yet
- Intra-Articular Fractures of Distal Humerus Managed With Anatomic Pre-Contoured Plates Via Olecranon Osteotomy ApproachDocument7 pagesIntra-Articular Fractures of Distal Humerus Managed With Anatomic Pre-Contoured Plates Via Olecranon Osteotomy ApproachIJAR JOURNALNo ratings yet
- Modified French OsteotomyDocument5 pagesModified French OsteotomyKaustubh KeskarNo ratings yet
- Salman-Outcome of Tendon Transfer Surgery For Radial NerveDocument4 pagesSalman-Outcome of Tendon Transfer Surgery For Radial NerveArief Setyo NugrohoNo ratings yet
- El BatrawypaperDocument7 pagesEl BatrawypaperabdallahalshallNo ratings yet
- The Results of Arthroscopic Release With Tendon Transfers in Cases of B.P.B.P With Glenohumeral DysplasiaDocument12 pagesThe Results of Arthroscopic Release With Tendon Transfers in Cases of B.P.B.P With Glenohumeral DysplasiaIJAR JOURNALNo ratings yet
- Ijos ArticleDocument5 pagesIjos ArticleReena RaiNo ratings yet
- 4 in 1 Quadricepsplasty For Fixed and Habitual DisDocument8 pages4 in 1 Quadricepsplasty For Fixed and Habitual DisMinh ChíNo ratings yet
- Reconstruction of Mandible by Free Fibular Flap: Original ArticleDocument5 pagesReconstruction of Mandible by Free Fibular Flap: Original ArticleSani Solihatul FitriNo ratings yet
- Ferran Ankle InstabilityDocument8 pagesFerran Ankle Instabilityfahmiatul lailiNo ratings yet
- 690 FullDocument8 pages690 Fulldanielalexandersinaga.xiiipa2No ratings yet
- Successful Outcome With Minimally Invasive Plate Osteosynthesis For Periprosthetic Tibial Fracture After Total Knee ArthroplastyDocument6 pagesSuccessful Outcome With Minimally Invasive Plate Osteosynthesis For Periprosthetic Tibial Fracture After Total Knee ArthroplastyMohebNo ratings yet
- J Clin Orthop Trauma 2021 20 101480Document8 pagesJ Clin Orthop Trauma 2021 20 101480Lucas SanchezNo ratings yet
- Should All Unstable Slipped Capital Femoral Epiphysis Be Treated OpenDocument7 pagesShould All Unstable Slipped Capital Femoral Epiphysis Be Treated Openyarimar hoyosNo ratings yet
- Adler 2007Document11 pagesAdler 2007Anand KarnawatNo ratings yet
- Posterior-Only Vertebral Column Resection For Fused SpondyloptosisDocument12 pagesPosterior-Only Vertebral Column Resection For Fused Spondyloptosisshivaprasad kolurNo ratings yet
- Arthroscopic Osseous Bankart Repair For Chronic Recurrent TraumaticDocument12 pagesArthroscopic Osseous Bankart Repair For Chronic Recurrent TraumaticdrjorgewtorresNo ratings yet
- Vandijk 2019 JJJJHHDocument9 pagesVandijk 2019 JJJJHHBeatriz GuimarãesNo ratings yet
- MPFL Rehab ProtocolDocument18 pagesMPFL Rehab ProtocolharyskawdNo ratings yet
- Disorders of the Patellofemoral Joint: Diagnosis and ManagementFrom EverandDisorders of the Patellofemoral Joint: Diagnosis and ManagementNo ratings yet
- Mcginley 2009Document10 pagesMcginley 2009Fernanda AhumadaNo ratings yet
- Bone Tumors Reconstructed Using Distraction OsteogenesisDocument9 pagesBone Tumors Reconstructed Using Distraction OsteogenesisFernanda AhumadaNo ratings yet
- Bone Transport For ReconstructionDocument6 pagesBone Transport For ReconstructionFernanda AhumadaNo ratings yet
- Bone Transport For ReconstructionDocument6 pagesBone Transport For ReconstructionFernanda AhumadaNo ratings yet
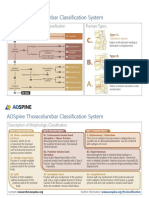
- AOSpine Thoracolumbar Classification System - PosterDocument1 pageAOSpine Thoracolumbar Classification System - PosterFernanda AhumadaNo ratings yet
- AOSpine Thoracolumbar Classification System - Pocket CardDocument2 pagesAOSpine Thoracolumbar Classification System - Pocket CardFernanda Ahumada0% (1)
- EndometriosisDocument153 pagesEndometriosisoannny8661No ratings yet
- Anti-Protozoal Drugs FinalizedDocument54 pagesAnti-Protozoal Drugs FinalizedMoazama Fayyaz100% (1)
- CVDocument3 pagesCVMaria InayatNo ratings yet
- Tenets and Codes of ConductDocument128 pagesTenets and Codes of ConductRodolf Dominic Serafin R. RobledoNo ratings yet
- Techniques For Parasite Egg Identification in Faecal SamplesDocument9 pagesTechniques For Parasite Egg Identification in Faecal SamplesDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU Philippines100% (2)
- DentistDocument3 pagesDentistuhurtuyNo ratings yet
- Times Leader 07-25-2011Document27 pagesTimes Leader 07-25-2011The Times LeaderNo ratings yet
- AP Research PresentationDocument26 pagesAP Research PresentationCameron SherryNo ratings yet
- PLI Proposal FormDocument8 pagesPLI Proposal FormPalakala NagarjunaNo ratings yet
- Traction PDFDocument31 pagesTraction PDFrushaliNo ratings yet
- Chalcone Synthesis, Structure DiversityDocument13 pagesChalcone Synthesis, Structure DiversityDini Elsi ANo ratings yet
- AlprazolamDocument10 pagesAlprazolamWen SilverNo ratings yet
- Ujian Akhir Semester Susulam Basic EnglishDocument15 pagesUjian Akhir Semester Susulam Basic EnglishNadia 13No ratings yet
- Torque in Orthodontics A Review March 2022 7544320615 0608221Document3 pagesTorque in Orthodontics A Review March 2022 7544320615 0608221chaitreeNo ratings yet
- Pain ADocument19 pagesPain Akcc2012No ratings yet
- OB Gyne HistoryDocument2 pagesOB Gyne HistoryNeil Victor Ongco PajugotNo ratings yet
- Traditional System of MedicineDocument5 pagesTraditional System of MedicinePriya SinghNo ratings yet
- Pemanfaatan Teknik Assisted Hatching Dalam Meningkatkan Implantasi EmbrioDocument10 pagesPemanfaatan Teknik Assisted Hatching Dalam Meningkatkan Implantasi EmbrioMumutTeaNo ratings yet
- MR Shyam OD 21.5 T3Document2 pagesMR Shyam OD 21.5 T3SaidasNo ratings yet
- Source: Bioethics Topics: Exam Questions & Answers Legal Medicine & Medical EthicsDocument67 pagesSource: Bioethics Topics: Exam Questions & Answers Legal Medicine & Medical Ethicsjamestery0% (1)
- Outbreak Investigation Part 1 PDFDocument4 pagesOutbreak Investigation Part 1 PDFashythegreat93No ratings yet
- Optimization of Granulation and Compression Process Variables of Atenolol Tablets Using Box Behnken DesignDocument9 pagesOptimization of Granulation and Compression Process Variables of Atenolol Tablets Using Box Behnken DesignnkszoneNo ratings yet
- Procalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsDocument2 pagesProcalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsMr. LNo ratings yet
- Turkey Tail MushroomDocument10 pagesTurkey Tail Mushroomjuanitos111100% (2)
- MEDDRA, PVPI, PVMF, PsMF-1Document28 pagesMEDDRA, PVPI, PVMF, PsMF-1Nitin Shah100% (1)
- Process RecordingDocument12 pagesProcess RecordingIanna J. L. PedrosaNo ratings yet
- Pharmacy Practice Sample ReportDocument26 pagesPharmacy Practice Sample Reportsaransh misraNo ratings yet
- Materi IAI Palangka Raya - Rev PDFDocument55 pagesMateri IAI Palangka Raya - Rev PDFNopernas CahayaNo ratings yet
- 11th Grade Before Band Aids TextDocument1 page11th Grade Before Band Aids Textعبدالرحمن باجسيرNo ratings yet