Professional Documents
Culture Documents
Evolucion Resistencia en Gram Positivos 2015 PDF
Uploaded by
Gustavo UrriagoOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Evolucion Resistencia en Gram Positivos 2015 PDF
Uploaded by
Gustavo UrriagoCopyright:
Available Formats
SUPPLEMENT ARTICLE
Evolving Resistance Among Gram-positive
Pathogens
Jose M. Munita,1,5,7 Arnold S. Bayer,3,4 and Cesar A. Arias1,2,5,6
1
Division of Infectious Diseases, Department of Internal Medicine, and 2Department of Microbiology and Molecular Genetics, University of Texas Medical
School at Houston; 3Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, Torrance, and 4David Geffen School of Medicine at UCLA,
Los Angeles, California; 5International Center for Microbial Genomics, and 6Molecular Genetics and Antimicrobial Resistance Unit, Universidad El Bosque,
Bogota, Colombia; and 7Clinica Alemana de Santiago, Universidad del Desarrollo, Chile
Antimicrobial therapy is a key component of modern medical practice and a cornerstone for the development of
complex clinical interventions in critically ill patients. Unfortunately, the increasing problem of antimicrobial
resistance is now recognized as a major public health threat jeopardizing the care of thousands of patients
worldwide. Gram-positive pathogens exhibit an immense genetic repertoire to adapt and develop resistance
to virtually all antimicrobials clinically available. As more molecules become available to treat resistant
gram-positive infections, resistance emerges as an evolutionary response. Thus, antimicrobial resistance has
to be envisaged as an evolving phenomenon that demands constant surveillance and continuous efforts to iden-
tify emerging mechanisms of resistance to optimize the use of antibiotics and create strategies to circumvent this
problem. Here, we will provide a broad perspective on the clinical aspects of antibiotic resistance in relevant
gram-positive pathogens with emphasis on the mechanistic strategies used by these organisms to avoid being
killed by commonly used antimicrobial agents.
Keywords. antimicrobial resistance; multidrug-resistant; methicillin-resistant; vancomycin-resistant;
penicillin-resistant.
The discovery and commercialization of antimicrobials that failure to tackle it could jeopardize modern medical
revolutionized modern medicine and became a major achievements [2].
tool for the development of complex medical interven- MDR gram-positive organisms are major human
tions, such as cancer therapy, organ transplantation, pathogens, causing both healthcare- and community-
and management of the critically ill. Unfortunately, an- associated infections. Among them, methicillin-resistant
timicrobial resistance is now threatening the care of Staphylococcus aureus (MRSA), vancomycin-resistant
such patients. Indeed, infections caused by multidrug- Enterococcus faecium (VRE), and drug-resistant Strep-
resistant (MDR) organisms are associated with signi- tococcus pneumoniae have been designated as serious
ficant mortality and carry an important economic public threats by the US Centers for Disease Control
burden, estimated at >$20 billion per year, just in the and Prevention [1]. Indeed, MRSA and VRE are lead-
United States [1]. Furthermore, the World Health Orga- ing causes of healthcare-associated infections in the
nization has identified antimicrobial resistance as one of United States, with conservative estimates suggesting
the most serious health threats worldwide and suggested they cause >12 000 deaths per year. Similarly, infections
due to drug-resistant S. pneumoniae, the main cause of
bacterial pneumonia and meningitis in adults, are esti-
Correspondence: Cesar A. Arias, MD, PhD, University of Texas Medical School at mated to cause 19 000 excess admissions and 7000
Houston, 6431 Fannin St, MSB 2.112, Houston, TX 77030 (cesar.arias@uth.tmc. deaths per year in the United States alone [1].
edu).
Clinical Infectious Diseases® 2015;61(S2):S48–57 The genetic and biochemical bases of antimicrobial
© The Author 2015. Published by Oxford University Press on behalf of the Infectious resistance in gram-positive bacteria are diverse and
Diseases Society of America. All rights reserved. For Permissions, please e-mail:
journals.permissions@oup.com.
they frequently differ within genera and/or species.
DOI: 10.1093/cid/civ523 Further, evolution of bacterial resistance is tightly
S48 • CID 2015:61 (Suppl 2) • Munita et al
influenced by the presence of environmental stressors, among inoculum (107 colony-forming units/mL) compared with the
which the use (and misuse) of antimicrobials is thought to standard inoculum (105 colony-forming units/mL). Although
play a major role. For instance, exposure of S. pneumoniae to the clinical relevance of this phenomenon is still controversial,
antibiotics has been shown to activate the transcription of a some evidence suggests that this phenotype may have important
gene regulon that results in increased genetic exchange with clinical implications in high-inocula infections, such as infective
co-colonizing organisms and the subsequent development of endocarditis [5–7].
resistant strains [3]. In this article, we will focus on the mecha- The mechanism of methicillin resistance relies on acquisition of
nisms of resistance in clinically important gram-positive bacte- the staphylococcal chromosomal cassette mec (SCCmec) contain-
ria, with emphasis on the most relevant antimicrobials used to ing mecA, which encodes PBP2a, a transpeptidase with low affin-
manage severe infections caused by these organisms. ity for all β-lactams (except for last-generation cephalosporins).
Expression of mecA is tightly regulated and it often requires in-
β-LACTAM RESISTANCE duction by a β-lactam. There are a number of different variants
of the SCCmec DNA; however, in general, shorter elements that
β-lactams disrupt cell-wall synthesis by mostly inhibiting lack resistance determinants to other antimicrobials are present in
transpeptidase activity of penicillin-binding proteins (PBPs) community-associated MRSA (SCCmec IV or V) [8].
that cross-link the nascent peptidoglycan. Penicillin resistance Ceftaroline and ceftobiprole are new additions to the β-lactam
was described shortly after penicillin discovery, prompting the family with potent activity against MRSA because of their enhanced
search for novel and more potent β-lactams. However, the dis- affinity for PBP2a. Ceftaroline resistance (MIC ≥4 μg/mL) in
covery of each new β-lactam compound has been consistently clinical MRSA is uncommon to date, but reports of isolates with
followed by emergence of resistance, highlighting that antimi- MICs between 4 and 8 μg/mL have been published [9–11], al-
crobial pressure is a major driving force of bacterial evolution. though the mechanisms leading to this phenotype are unclear.
There are 2 main mechanisms of β-lactam resistance in gram- During 2014, an MRSA isolate with a high ceftaroline MIC
positive pathogens, enzymatic degradation through the produc- (>32 μg/mL; ST5) was recovered from the bloodstream of a pa-
tion of β-lactamases and decreased affinity of the antibiotic for tient previously treated with ceftaroline in Houston, Texas. The
its target, usually either by acquisition of exogenous DNA encod- mechanism of resistance was associated with 2 contiguous sub-
ing a low-affinity PBP or through changes in the native pbp genes stitutions (Y446N and E447K) in the penicillin-binding pocket
(Table 1). of the transpeptidase domain of PBP2a [12]. Interestingly, the
E447K substitution had been previously selected in vitro by cef-
β-Lactam Resistance in S. aureus tobiprole passage [13].
Emergence and dissemination of β-lactam resistance in S. aure-
us occurred in several epidemic waves that could be summa- β-Lactam Resistance in Enterococci
rized by (1) acquisition of a plasmid-encoded penicillinase in Treatment of enterococcal infections has long been considered a
the 1950s ( particularly the clone known as phage type 80/81), therapeutic challenge. Indeed, the MICs of penicillin and ampi-
(2) a second wave that started after the introduction of methi- cillin (the most active anti-enterococcal β-lactams) are much
cillin (1959) and was characterized by the emergence of hospi- higher than for other common gram-positive organisms, prob-
tal-associated MRSA isolates that mainly circulated in European ably owing to the expression of lower affinity PBPs (eg, PBP5),
hospitals until the 1970s, (3) the development of several highly and enterococcal isolates are often tolerant to β-lactam antibi-
successful hospital-associated MRSA clones that spread in otics (ie, lack of bactericidal activity in vitro), complicating the
different parts of the world, and continue to circulate (third treatment of serious infections [14]. Furthermore, high-level
wave), and (4) the last wave of MRSA resistance to date, charac- resistance to ampicillin (MICs ≥64 μg/mL) is a hallmark of
terized by the emergence and dissemination of community- healthcare-associated MDR isolates of E. faecium. Conversely,
associated MRSA in the 1990s [4]. Nowadays, most S. aureus ampicillin resistance continues to be strikingly uncommon in
are penicillin-resistant through the production of a plasmid- Enterococcus faecalis isolates.
borne β-lactamase (4 types are known, including A, B, C, and D). The mechanisms of high-level ampicillin resistance in en-
Although the anti-staphylococcal penicillins (eg, nafcillin) terococci are not completely understood but they have been
are stable against these enzymes, staphylococcal-type A β-lactamase most consistently associated with changes in the pbp5 gene, en-
has higher rates of cefazolin hydrolysis, and some methicillin- coding a PBP with low affinity for β-lactams [15]. A variety of
susceptible S. aureus (MSSA) isolates harboring this enzyme ex- mutations have been described and although the individual
hibit the so-called cefazolin inoculum effect. This phenomenon contribution to resistance of each genetic change is unclear, some
involves increased minimum inhibitory concentrations (MICs) of them (eg, M485A plus insertion of Ser466) have been directly
to cefazolin when susceptibility testing is performed using a higher linked to the resistance phenotype [16]. In addition, studies on
Gram-positive Resistance • CID 2015:61 (Suppl 2) • S49
Table 1. Resistance Mechanisms in Clinically Important Gram-positive Pathogens
Pathogen and
Resistance Strategy Antibiotic Gene(s) Involved Comments
Staphylococci
Drug inactivation β-lactams (penicillins with blaZ Plasmid-encoded β-lactamase that hydrolyzes penicillins;
or without cefazolina) isoxazolyl penicillins (eg, nafcillin), cephalosporins,a and
carbapenems are stable
Target replacement β-lactams mecA PBP2a has low affinity for β-lactams (except ceftaroline and
ceftobiprole)
Vancomycin (VRSA) vanA Gene cluster Acquired from enterococci; rare isolates described
Target modification Linezolid 23S rRNA genes, L3/L4 Mutations in 23S rRNA genes are main mediators of
ribosomal proteins resistance; cfr gene is the only transferable determinant
cfr of LNZ-R
Ceftaroline pbp2a Mutations in pbp2a associated with high-level ceftaroline
resistance (MIC >32 µg/mL)
Changes in cell Vancomycin (VISA) vraRS, yycFG, graRS, rpoB Many genes involved in the resistance phenotype, most
surface related to regulatory systems
adaptation Daptomycin mprF, dlt, Many genes involved in the resistant phenotype; main
vraRS, yycFG, pgsA, cls pathway seems to be repulsion of the antibiotic through
an increase in the net positive charge of the cell envelope
Enterococci
Drug inactivation β-lactams (penicillins) blaZ Rare, found mostly in E. faecalis
Target replacement Vancomycin van Gene clusters Several gene clusters described, most acquired on mobile
elements; intrinsic low-level resistance seen in
E. gallinarium and E. casseliflavus (VanC phenotype)
Target modification β-lactams (penicillin and pbp5 b PBP5-R differs from PBP5-S in only about 5% of amino acid
ampicillin) sequence; certain amino acid substitutions have been
directly implicated in ampicillin resistance (see text)
Linezolid 23S rRNA genes, L3/L4 Rare, mutations in 23S rRNA and L3/L4 are similar to those
ribosomal proteins, cfr found in staphylococci, as is the cfr gene
Changes in cell Daptomycin liaFSR, yycGF, gdpD, Most frequent mutations found in daptomycin-resistant
surface cls clinical isolates; many genes involved; resistance
adaptation pathways differ between E. faecalis and E. faecium
Streptococci
Target modification β-lactams (penicillin) PBPs (pbp2x, pbp2b in PBP changes are the most important determinant of
pneumococci), β-lactam resistance; mosaic PBPs are often found in
murM, cpoA, pdgA penicillin-resistant isolates
Linezolid 23S rRNA genes, L3/L4 Rare
ribosomal proteins, cfr
Unknown Daptomycin Unknown Rapid development of daptomycin resistance in certain
species of streptococci
Abbreviations: LNZ-R, linezolid resistance; MIC, minimum inhibitory concentration; PBP, penicillin-binding protein; rRNA, ribosomal RNA; VISA, vancomycin-
intermediate Staphylococcus aureus; VRSA, vancomycin-resistant S. aureus.
a
The ability of certain types of staphylococcal β-lactamase to hydrolyze cefazolin may cause therapeutic failures.
b
PBP5 (encoded by pbp5) is part of the core genome of enterococci. Because of its decreased affinity for penicillin, it is responsible for the natural tolerance of these
organisms to β-lactams.
sequence variation of the pbp5 allele identified specific differ- low over the years and has been described in only a few E. fae-
ences between ampicillin-susceptible and ampicillin-resistant cium isolates [18].
isolates (harboring pbp5-S and pbp5-R alleles, respectively),
suggesting evolutionary adaptation [17]. Indeed, PBP5-R and β-Lactam Resistance in Pneumococci
PBP5-S sequences differ in approximately 5%, at the amino Streptococcus pneumoniae is naturally susceptible to most anti-
acid level, although no particular change has been consistently microbials, including penicillins, long considered the first-line
correlated with specific increases in the ampicillin MIC. Finally, therapy for pneumococcal infections. Current Clinical and Lab-
β-lactamase–mediated ampicillin resistance has also been de- oratory Standards Institute break points for parenteral penicil-
scribed in enterococcal isolates. Initially found in E. faecalis in lin establish that isolates not causing meningitis are categorized
the early 1980s, the frequency of this mechanism has remained as susceptible, intermediate, or resistant, with MICs of ≤2, 4,
S50 • CID 2015:61 (Suppl 2) • Munita et al
and ≥8 μg/mL, respectively [19]. In contrast, meningitis isolates challenging causes of healthcare-associated infections. Impor-
are considered penicillin susceptible (MIC ≤0.06 μg/mL) or re- tantly, there are considerable interspecies differences, with
sistant (≥0.12 μg/mL) [19]. The first significant outbreak of most vancomycin resistance occurring in E. faecium isolates
penicillin-resistant S. pneumoniae was reported in the 1970s [26]. The successful spread of E. faecium has been tracked to
and, since then, their frequency has steadily increased world- the dissemination of a hospital-associated genetic clade that is
wide [20]. Prevalences of β–lactam-resistant pneumococci often MDR, also harboring ampicillin and high-level aminogly-
vary widely within different regions and are largely shaped by coside resistance determinants [27].
the use patterns of conjugated pneumococcal vaccines [21]. The mechanism of VRE is acquisition of van gene clusters,
The main mechanism of pneumococcal β-lactam resistance is probably from environmental organisms. The most frequent
through changes in the native PBPs by recombination with ex- gene cluster is vanA, usually located in a Tn3-family transposon
ogenous pbp genes, in a process that relies on the pneumococcal (Tn1546) that has been found in conjugative and nonconju-
ability to incorporate naked DNA from the environment (trans- gative plasmids. In addition, 8 other van clusters (vanBC-
formation). Point mutations in pbp genes also play a role and DEGLMN) have been characterized in enterococcal isolates.
may act synergistically to further increase the MICs. Recombi- These gene clusters encode a complex enzymatic machinery
nant PBPs of resistant isolates are highly variable and classically that modifies the terminal D-Ala-D-Ala termini of peptidogly-
show mosaic blocks that derive from the recombination with can precursors and destroys the “normal” D-Ala-D-Ala ending
external pbp genes (mostly from Streptococcus mitis and Strep- precursors. Most frequently, D-Ala-D-Ala is replaced for
tococcus oralis) [22, 23]. Strikingly, the magnitude of the recom- D-Ala-D-lactate, decreasing the affinity of vancomycin for its
bination can be such that it may change the serotype of the target by approximately 1000-fold. D-Ala-D-Ala can also be
isolate. Mosaicism in PBP2x and PBP2b is the most frequent replaced for D-Ala-D-serine, which affects the affinity of vanco-
change associated with β-lactam resistance. Moreover, muta- mycin for its target to a lesser degree (resulting in relatively low-
tional changes in PBP1a can result in high-level resistance level resistance, with MICs of 4–32 μg/mL).
when they occur in the background of low-affinity mosaic In general, the van clusters harbor 3 classes of genes: those
PBP2x or PBP2b [24]. Alterations in the remaining PBPs have encoding a 2-component regulatory system that tightly controls
been occasionally related to resistance, but their frequency is the expression of the resistance genes, those involved in the
lower. Finally, mutations in other genes, such as murM (in- biochemical pathway for synthesis of D-lactate or D-serine,
volved in the biosynthesis of the murein), pdgA (encoding a and those involved in the destruction of normal D-Ala-D-
GlcNAc deacetylase), and cpoA (that codes for a glycosyltrans- Ala-ending peptidoglycan precursors, encoding proteins with
ferase) have also been uncommonly associated with β-lactam dipeptidase and carboxypeptidase activities. The biochemical
resistance in pneumococci [24]. pathways of vancomycin resistance in enterococci have been ex-
tensively described [28], and a detailed explanation is beyond
GLYCOPEPTIDE RESISTANCE the scope of this review.
Glycopeptides prevent cross-linking of peptidoglycan by bind- Vancomycin Resistance in Staphylococci
ing to the terminal D-alanine-D-alanine (D-Ala-D-Ala) of Reduced vancomycin susceptibility in staphylococci can be cat-
peptidoglycan precursors, inhibiting cell-wall synthesis. Vanco- egorized by 2 distinct phenotypes: (1) most commonly, isolates
mycin was first approved for clinical use in 1958, and for many with intermediate susceptibility to vancomycin (vancomycin-
years has been the “workhorse” antibiotic for the treatment of intermediate S. aureus [VISA]; MIC, 4–8 μg/mL), and (2) rare-
MRSA infections. Despite its heavy use, it took >40 years for the ly, high-level resistance to vancomycin (vancomycin-resistant
first clinical isolates with high-level resistance to vancomycin to S. aureus [VRSA]; MIC ≥16 μg/mL) [29]. The first VISA isolate
emerge [25]. (Mu50), reported in 1997, was derived from a vancomycin-
susceptible strain (Mu3), later found to have a small subpopulation
Vancomycin-Resistant Enterococci with MICs >2 μg/mL, a condition now designated heterogeneous
VRE isolates were first described as community commensals in VISA or hetero-VISA (hVISA). The hVISA/VISA phenotype
1986 in Europe, and were associated with the use of avoparcin, a usually arises in vivo in patients with invasive staphylococcal in-
glycopeptide used in animal husbandry. Consequently, avopar- fections who received a prolonged course of vancomycin [30].
cin use was banned, and the frequency of VRE decreased. Later, Thus, although the overall prevalence of hVISA/VISA is low, it
VRE emerged in the United States (where avoparcin was never can reach up to 30% in selected clinical scenarios using refined
approved), mainly in clinical isolates recovered from the hospi- assays to detect resistant subpopulations (eg, patients with
tal environment. Since then, VRE prevalence in the United MRSA and infective endocarditis) [31]. Outbreaks caused by
States has steadily increased, becoming one of the most hVISA/VISA strains have also been reported, but their occurrence
Gram-positive Resistance • CID 2015:61 (Suppl 2) • S51
continues to be sporadic [32]. Interestingly, the VISA pheno- compounds inhibit protein synthesis through interactions
type has also been described in a minority of MSSA strains. with the A site of the 50S ribosomal subunit. Mechanisms of
Although the genetic basis of hVISA/VISA seems to be complex oxazolidinone resistance include (1) mutations in the genes en-
and not completely understood, the available evidence suggests coding the 23S ribosomal RNA (rRNA), (2) changes in the L3/
that it requires a number of ordered and sequential mutations L4 ribosomal proteins, and (3) methylation of the 23S rRNA by
that usually involve several regulatory systems controlling cell- a methylase designated as Cfr (chloramphenicol-florfenicol re-
envelope homeostasis [33]. Among them, the genes most con- sistance) (Figure 1). Overall, mutations in the central loop of the
sistently implicated are walkR (also known as yycFG), vraRS domain V of the 23 rRNA are the most frequent determinants
(homolog of liaFSR), and graRS [34, 35]. Mutations in rpoB of linezolid resistance (LNZ-R). Although several mutations
(encoding the RNA polymerase subunit B) have also been linked have been described, the most frequent change found in clinical
with the VISA phenotype. These genetic changes produce impor- isolates is G2576T (Escherichia coli numbering). Importantly,
tant remodeling of the cell envelope, resulting in a thickened cell because bacteria carry multiple copies of the 23S rRNA genes,
wall that seem to harbor increased amounts of free D-Ala-D-Ala mutations need to accumulate in several copies to increase the
dipeptides with reduced cross-linking [30]. Overall, these pertur- MIC (gene-dose effect) [43]. Substitutions in the L3 and L4 ri-
bations may “trap” vancomycin in outer layers of the peptidogly- bosomal proteins are also associated with development of LNZ-
can, preventing its ability to reach its target of peptidoglycan R in vivo and in vitro, both alone and in combination with other
precursors emerging from the cytoplasm. resistance determinants. Interestingly, mutations in the L3/L4
The first reported case of VRSA occurred in Michigan in seem to be particularly frequent in coagulase-negative staphylo-
2002 and resulted from the acquisition of the vanA gene cluster cocci (see below).
from a vancomycin-resistant E. faecalis [36]. However, in con- Cfr encodes a methyltransferase whose target is position
trast to VRE, VRSA remain rare, with only 13 isolates described A2503 of the 23S rRNA. Initially reported in a Staphylococcus
in the United States and a total of 4 additional cases reported sciuri recovered from cattle, cfr was first described in humans in
from Brazil, Portugal, Iran, and India [33, 37]. Most VRSA 2005 in a S. aureus isolated from a patient in Colombia [44].
strains have been recovered as “colonizers” from the skin of di- Since then, it has been found in several bacterial species. Over-
abetic patients; 12 of the 13 cases found in the United States all, cfr carriage continues to be sporadic, however, areas of en-
correspond to MRSA belonging to CC5, the most common demicity have been reported [45]. Furthermore, cfr-positive
clonal complex associated with MRSA hospital dissemination isolates have been associated with outbreaks of LNZ-R S. aureus
in the country (the remaining isolate belongs to CC30). Impor- and coagulase-negative staphylococci in different clinical set-
tantly, a Brazilian MRSA isolate carrying the vanA gene cluster tings [46, 47]. Cfr is the only transmissible LNZ-R determinant
(ST8) was found to be related to a community-associated MRSA and it has been associated with various mobile genetic elements.
genetic lineage with high dissemination capacity in Latin Amer- In addition, it is frequently cotransmitted with other resistance
ica (USA300, Latin American variant). Most worrisome, the determinants that affect protein synthesis, and it seems to carry
vanA gene cluster in this isolate was found in a highly transfer- a low fitness cost [48]. Altogether, these characteristics suggest
able staphylococcal plasmid that was also acquired by a different that the potential for dissemination of this MDR trait is high. It
bloodstream isolate of MSSA within the same patient [37]. is also important to note that in contrast to mutational resis-
Finally, 3 antibiotics from the lipoglycopeptide family have tance, in vivo data suggested that cfr-mediated LNZ-R could
been approved by the US Food and Drug Administration for be overcome with higher doses of the antibiotic [49]. Important-
the treatment of gram-positive infections, namely, telavancin ly, carriage of cfr does not seem to confer resistance to tedizolid,
[38], dalbavancin [39] and oritavancin [40]. All of these com- the other oxazolidinone approved in 2014 by the Food and
pounds appear to be active in vitro against hVISA/VISA isolates. Drug Administration for the treatment of skin and soft-tissue
Of these 3 drugs, oritavancin retains some in vitro activity against infections [50].
enterococcal strains exhibiting the VanA phenotype [41]. None-
theless, its clinical efficacy against these latter strains remains to LNZ-R in Staphylococci
be established, and initial studies in animal models suggest that Two comprehensive surveillances collecting worldwide isolates
selection of resistant mutants is likely when oritavancin is used over a 10-year-period showed that staphylococcal isolates have
as monotherapy [42]. remained highly susceptible to linezolid [45]. As mentioned,
changes in L3/L4 ribosomal proteins are particularly frequent
OXAZOLIDINONE RESISTANCE in Staphylococcus epidermidis, with 1 study finding them in 89
of 122 LNZ-R isolates (73%). In terms of frequency, cfr was pre-
Two oxazolidinones are currently available for the treatment of sent in 13% of S. aureus and in 15% of 182 LNZ-R coagulase-
gram-positive infections, namely linezolid and tedizolid. Both negative staphylococci from postmarketing surveillance [45]. In
S52 • CID 2015:61 (Suppl 2) • Munita et al
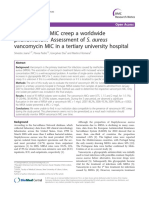
Figure 1. Schematic representation of the mechanism of action and resistance to linezolid. A, Linezolid interferes with the positioning of aminoacyl
transfer RNA (tRNA) by interactions with the peptidyl transferase center. Ribosomal proteins L3 and L4, associated with resistance, are shown.
B, Representation of domain V of 23S ribosomal RNA (rRNA) showing mutations associated with linezolid resistance. Position A2503, the target of Cfr
(chloramphenicol-florfenicol resistance) methylation, is highlighted. Abbreviation: mRNA, messenger RNA.
addition, several outbreaks of cfr-positive S. aureus and S. epi- Although cfr has been reported in clinical enterococcal isolates
dermidis have been reported, and a 2013 report implicated cfr in [54], its overall frequency continues to be low.
local endemicity of LNZ-R in a hospital in Madrid [51]. Tedi-
zolid resistance has been described in vitro, and the main mech- LNZ-R Streptococci
anism relates to changes in the 23S rRNA (including the Very few cases of LNZ-R streptococci have been described, in-
presence of a dual-mutation T2571C plus G2576T) [52]. cluding sporadic reports of LNZ-R S. pneumoniae, Streptococ-
cus sanguinis, and S. oralis. In addition, the cfr gene was
LNZ-R Enterococci reported from a Streptococcus suis isolate of porcine origin
The first described LNZ-R clinical isolates were E. faecium re- [55]. In a 2014 report, no resistance was found in 6691 pneumo-
covered from patients receiving linezolid as part of a compas- cocci, 2463 viridans streptococci, or 4153 β-hemolytic strepto-
sionate program. As seen in other bacteria, the prevalence of cocci [53].
LNZ-R enterococci has remained low. Data from 6718 entero-
coccal isolates tested from 2004 to 2012 showed that the preva- DAPTOMYCIN RESISTANCE
lence of LNZ-R consistently remained <0.9% [53]. Mutations in
the 23S rRNA genes are the most frequently identified changes. Daptomycin (DAP) is a bactericidal lipopeptide antibiotic ac-
In fact, of 48 LNZ-R E. faecalis and 121 E. faecium, these tive against a wide range of gram-positive clinical pathogens.
mutations were the only identified resistance trait in 73% and It damages the cell membrane (CM) in a calcium-dependent
88% of isolates, respectively [45]. Furthermore, only 3 E. faeci- manner, interacting with its target mostly at the bacterial
um isolates harbored changes in the L3/L4 ribosomal proteins. division septum. Importantly, the presence of specific CM
Gram-positive Resistance • CID 2015:61 (Suppl 2) • S53
phospholipids (eg, phosphatidylglycerol [PG]) is crucial for to PG. The resulting lysyl-PG, a positively charged phospholip-
the antibacterial action of DAP [56, 57]. Development of DAP id, is translocated from the inner to the outer leaflet of the CM
resistance (DAP-R) during therapy seems to be an important by the same enzyme [61].
problem affecting the clinical efficacy of DAP. The exact mech- Several mprF mutations have been associated with DAP-R,
anisms of DAP-R remain to be elucidated, but current knowl- most frequently producing a “gain of function” phenotype.
edge suggests that they are complex, diverse, and multifactorial, The increased positive charge of the cell envelope is thought
arising from mutational changes (Table 1). to impair the binding of DAP to the CM target. The DAP re-
pulsion theory has also been supported by the finding of DAP-
DAP-R in S. aureus R strains overexpressing the dlt operon, responsible for the
Most S. aureus remain DAP susceptible (DAP-S), but reports incorporation of D-alanine ( positively charged amino acid) into
documenting the emergence of DAP-R continue to accumulate, cell-wall teichoic acids [62]. However, repulsion is not the only
particularly in the context of high-inoculum infections and/or explanation for DAP-R staphylococci, because not all isolates
after exposure to vancomycin [58, 59]. It has been postulated with mprF mutations exhibit significant changes in surface
that the mechanism of DAP-R in S. aureus is mediated by elec- charge, and DAP-R isolates with either no mutations in mprF
trostatic repulsion of the DAP calcium complex from the cell or without gain in function in the enzyme have been described.
surface, mainly by increasing the positive charge of the bacterial Other determinants implicated in DAP-R include genes en-
surface [60] (Figure 2). The most common gene implicated in coding enzymes involved in phospholipid metabolism, such PG
the phenotype is mprF, which encodes a bifunctional enzyme and cardiolipin synthetases ( pgsA and cls, respectively) [63]. In
(MprF) that incorporates the positive charged amino acid lysine addition, DAP-R isolates seem to exhibit important changes in
Figure 2. Proposed mechanisms of action and resistance to daptomycin in Gram-positive organisms. A, The daptomycin-calcium complex interacts with
the cell membrane mainly at septal areas. B, In Enterococcus faecalis, the antibiotic is diverted from the septum (black arrow) in a process associated with
redistribution of anionic phospholipid microdomains (eg, cardiolipin) away from the septal plane. C, In Staphylococcus aureus and Enterococcus faecium, the
positively charged daptomycin-calcium complex is “repelled” from the cell surface in a process associated with increase in the net positive charge of the
cell envelope (not all strains). Abbreviations: DAP-R, daptomycin-resistant; DAP-S, daptomycin-susceptible.
S54 • CID 2015:61 (Suppl 2) • Munita et al
cell-wall homeostasis, similar to those observed in VISA iso- therapeutic failure, irrespective of the MIC [69]. Of note, a
lates. The 2-component regulatory systems VraSR and YycFG 2014 report of DAP failure in a patient with VRE bacteremia
(WalKR) are thought to play a particularly important role in de- caused by a DAP-S isolate (MIC, 3 μg/mL) harboring liaFSR
velopment of DAP-R [59]. Indeed, mutations in yycFG have mutations further supports the role of these genes in the
been directly implicated in DAP-R, and inactivation of vraSR DAP-R phenotype [70].
in a DAP-R isolate caused reversion to DAP-S [64]. Interesting-
ly, 1 study showed that up to 80% of VISA isolates were DAP-R DAP-R in Streptococci
[59, 65]. In addition, DAP-R emerged in a patient with MRSA Reports of DAP-R streptococcal strains are rare, and large sur-
endocarditis in whom vancomycin therapy failed after a VISA veillance programs consistently show that streptococcal isolates
phenotype developed, although never exposed to DAP [35]. remain almost uniformly susceptible to DAP. Importantly, re-
cent evidence suggests that high-level and durable DAP-R can
DAP-R in Enterococci rapidly arise in vivo and in vitro when viridans group strepto-
Enterococci are less susceptible than staphylococci to DAP cocci are exposed to DAP [71, 72]. However, the actual mecha-
(Clinical and Laboratory Standards Institute break point, 4- nism of this form of DAP-R has not been elucidated.
fold that of S. aureus). Most genes implicated in DAP-R in en- Development of DAP-R seems to be correlated with an in-
terococci seem to be grouped into 2 broad categories: those creased susceptibility to β-lactam antibiotics (“see-saw” effect)
encoding regulatory systems that orchestrate cell-envelope ho- [73]. Indeed, several reports have suggested that the DAP-β-
meostasis and stress response and those coding for enzymes lactam combination is efficacious and bactericidal against
involved in CM phospholipid metabolism. Interestingly, the DAP-R isolates [73–76]. Although the mechanism of this ap-
mechanisms of DAP-R seem to differ between E. faecium and parent synergy has not been fully elucidated, it seems to be
E. faecalis (Figure 2). dependent on specific PBPs (ie, PBP-1 in S. aureus) [77] and
Genomic analysis of a clinical strain pair of E. faecalis iden- on the genetic pathway leading to the DAP-R phenotype [78].
tified 3 genes responsible for DAP-R in vivo [66]. Two of them
(gdpD and cls encoding a phosphodiesterase and cardiolipin CONCLUSION
synthase, respectively) were involved in phospholipid metabo-
lism; the remaining locus (liaF) was part of a 3-component reg- Resistance to front-line antibiotics is an evolving phenomenon
ulatory system (LiaFSR, a homologue of the S. aureus VraTSR in gram-positive bacterial pathogens. Despite the availability of
system described above) that orchestrates the cell-envelope new molecules to treat infections caused by these organisms, the
stress response in gram-positive organisms. Changes in LiaFSR optimal therapeutic approaches remain to be established. The
are thought to be the initial and pivotal modifications contrib- immense genetic plasticity of the most clinically relevant
uting to the development of DAP-R in vivo. Furthermore, dele- gram-positive bacteria poses important challenges for designing
tion of liaR, the response regulator of the LiaFSR system, strategies to curtail development of resistance. As new com-
resulted in complete reversal of the DAP-R phenotype [67]. pounds become available, the adaptive bacterial response will
Most importantly, the mechanism of resistance does not seem probably emerge in clinical settings. Therefore, efforts to opti-
to be mediated by repulsion of the antibiotic from the cell sur- mize the use of antibiotics with gram-positive spectrum and
face; instead, the lack of killing by DAP has been best correlated identify emerging mechanisms of resistance should be clinical
with a “redistribution” of CM cardiolipin microdomains away priorities.
from the septum mediated by the LiaFSR system, a change that
seems to prevent the interaction of DAP with its main septal Notes
target (the “diversion” hypothesis; see Figure 2) [68]. In addi- Financial support. Editorial support, funded by Theravance Biophar-
tion, changes in the CM phospholipid composition (mainly de- ma Antibiotics, Inc, was provided by Envision Scientific Solutions. This
creased PG and increased cardiolipin) seem to be paramount in work was supported by the Chilean Ministry of Education, Clinical Alemana
de Santiago, and Universidad del Desarrollo School of Medicine, Chile
DAP-R in E. faecalis. (grants to J. M. M.); and by the National Institute of Allergy and Infectious
Recent evidence suggests that the “repulsion” mechanism is Diseases, National Institutes of Health (grants R01 AI39108–15 to A. S. B.
more likely to mediate DAP-R in E. faecium (Figure 2), al- and R01 AI093749 to C. A. A.).
Supplement sponsorship. This article was published as part of a
though the genetic basis of resistance appears to be similar to
supplement titled “Telavancin: Treatment for Gram-positive Infections–
that of E. faecalis. Furthermore, changes in LiaFSR were also fre- New Perspectives on In Vitro and Clinical Data,” sponsored by Theravance
quently found in DAP-S clinical E. faecium isolates with MICs Biopharma Antibiotics, Inc.
Potential conflicts of interest. The authors received no financial com-
close to the break point (3–4 μg/mL), and their presence was
pensation for the preparation of this article. A. S. B has provided expert tes-
sufficient to abolish the bactericidal activity of DAP. These timony to Johnson, Graffe, et al; Morrow, Kidman, Tinker, et al; Galloway,
data suggested that such mutations could increase the risk of Lucchese, et al; MES Solutions; Hoffman, Sheffield, et al; and Clifford
Gram-positive Resistance • CID 2015:61 (Suppl 2) • S55
Law. C. A. A. has received lecture fees, research support, and consulting fees 18. Murray BE, Mederski-Samaroj B. Transferable beta-lactamase: a new
from Pfizer; lecture and consulting honoraria from Novartis, Cubist, Forest mechanism for in vitro penicillin resistance in Streptococcus faecalis.
Pharmaceuticals, AstraZeneca and Bayer Pharmaceuticals; and research J Clin Invest 1983; 72:1168–71.
support from Forest Pharmaceuticals, Theravance, and Theravance Bio- 19. Clinical and Laboratory Standards Institute. MS100-22. Performance stan-
pharma Antibiotics, Inc. J. M. M. reports no potential conflicts. dards for antimicrobial susceptibility testing: 21st informational supplement.
All authors have submitted the ICMJE Form for Disclosure of Potential Vol. 32. Wayne, PA: Clinical and Laboratory Standards Institute, 2012.
Conflicts of Interest. Conflicts that the editors consider relevant to the con- 20. Jacobs MR, Koornhof HJ, Robins-Browne RM, et al. Emergence of mul-
tent of the manuscript have been disclosed. tiply resistant pneumococci. N Engl J Med 1978; 299:735–40.
21. Dagan R, Juergens C, Trammel J, et al. Efficacy of 13-valent pneumo-
coccal conjugate vaccine (PCV13) versus that of 7-valent PCV (PCV7)
References against nasopharyngeal colonization of antibiotic-nonsusceptible Strep-
tococcus pneumoniae. J Infect Dis 2015; 211:1144–53.
1. Centers for Disease Control and Prevention. Antibiotic resistance threats 22. Dowson CG, Coffey TJ, Kell C, Whiley RA. Evolution of penicillin re-
in the United States. Available at: http://www.cdc.gov/drugresistance/ sistance in Streptococcus pneumoniae; the role of Streptococcus mitis in
threat-report-2013/index.html. Accessed 9 March 2015. the formation of a low affinity PBP2B in S. pneumoniae. Mol Microbiol
2. World Health Organization. Antimicrobial resistance: global report on 1993; 9:635–43.
surveillance 2014. Available at: http://www.who.int/drugresistance/ 23. Sibold C, Henrichsen J, Konig A, Martin C, Chalkley L, Hakenbeck R.
documents/surveillancereport/en/. Accessed 4 March 2015. Mosaic pbpX genes of major clones of penicillin-resistant Streptococcus
3. Cornick JE, Bentley SD. Streptococcus pneumoniae: the evolution of an- pneumoniae have evolved from pbpX genes of a penicillin-sensitive
timicrobial resistance to beta-lactams, fluoroquinolones and macrolides. Streptococcus oralis. Mol Microbiol 1994; 12:1013–23.
Microbs Infect 2012; 14:573–83. 24. Hakenbeck R, Bruckner R, Denapaite D, Maurer P. Molecular mecha-
4. Chambers HF, Deleo FR. Waves of resistance: Staphylococcus aureus in nisms of beta-lactam resistance in Streptococcus pneumoniae. Future
the antibiotic era. Nat Rev Microbiol 2009; 7:629–41. Microbiol 2012; 7:395–410.
5. Bai AD, Showler A, Burry L, et al. Comparative effectiveness of cefazolin 25. Cattoir V, Leclercq R. Twenty-five years of shared life with vancomycin-
versus cloxacillin as definitive antibiotic therapy for MSSA bacteraemia: resistant enterococci: is it time to divorce? J Antimicrob Chemother
results from a large multicentre cohort study. J Antimicrob Chemother 2013; 68:731–42.
2015; 70:1539–46. 26. Arias CA, Murray BE. The rise of the Enterococcus: beyond vancomycin
6. Lee S, Kwon KT, Kim HI, et al. Clinical implications of cefazolin inoc- resistance. Nat Rev Microbiol 2012; 10:266–78.
ulum effect and beta-lactamase type on methicillin-susceptible Staphy- 27. Lebreton F, van Schaik W, McGuire AM, et al. Emergence of epidemic
lococcus aureus bacteremia. Microb Drug Resist 2014; 20:568–74. multidrug-resistant Enterococcus faecium from animal and commensal
7. Nannini EC, Singh KV, Arias CA, Murray BE. In vivo effect of cefazolin, strains. MBio 2013; 4:e00534–13.
daptomycin, and nafcillin in experimental endocarditis with a methicil- 28. Courvalin P. Vancomycin resistance in gram-positive cocci. Clin Infect
lin-susceptible Staphylococcus aureus strain showing an inoculum effect Dis 2006; 42(suppl 1):S25–34.
against cefazolin. Antimicrob Agents Chemother 2013; 57:4276–81. 29. Tenover FC, Moellering RC Jr. The rationale for revising the Clinical
8. DeLeo FR, Chambers HF. Reemergence of antibiotic-resistant Staphylo- and Laboratory Standards Institute vancomycin minimal inhibitory
coccus aureus in the genomics era. J Clin Invest 2009; 119:2464–74. concentration interpretive criteria for Staphylococcus aureus. Clin Infect
9. Mendes RE, Tsakris A, Sader HS, et al. Characterization of methicillin- Dis 2007; 44:1208–15.
resistant Staphylococcus aureus displaying increased MICs of ceftaro- 30. Howden BP, Davies JK, Johnson PD, Stinear TP, Grayson ML. Reduced
line. J Antimicrob Chemother 2012; 67:1321–4. vancomycin susceptibility in Staphylococcus aureus, including vanco-
10. Alm RA, McLaughlin RE, Kos VN, Sader HS, Iaconis JP, Lahiri SD. mycin-intermediate and heterogeneous vancomycin-intermediate
Analysis of Staphylococcus aureus clinical isolates with reduced suscept- strains: resistance mechanisms, laboratory detection, and clinical impli-
ibility to ceftaroline: an epidemiological and structural perspective. cations. Clin Microbiol Rev 2010; 23:99–139.
J Antimicrob Chemother 2014; 69:2065–75. 31. Bae IG, Federspiel JJ, Miro JM, et al; International Collaboration on
11. Kelley WL, Jousselin A, Barras C, Lelong E, Renzoni A. Missense mu- Endocarditis-Microbiology Investigators. Heterogeneous vancomycin-
tations in PBP2A affecting ceftaroline susceptibility detected in epidem- intermediate susceptibility phenotype in bloodstream methicillin-
ic hospital-acquired methicillin-resistant Staphylococcus aureus resistant Staphylococcus aureus isolates from an international cohort
clonotypes ST228 and ST247 in western Switzerland archived since of patients with infective endocarditis: prevalence, genotype, and clini-
1998. Antimicrob Agents Chemother 2015; 59:1922–30. cal significance. J Infect Dis 2009; 200:1355–66.
12. Long SW, Olsen RJ, Mehta SC, et al. PBP2a mutations causing high- 32. Parer S, Lotthe A, Chardon P, Poncet R, Jean-Pierre H, Jumas-Bilak E.
level ceftaroline resistance in clinical methicillin-resistant Staphylococ- An outbreak of heterogeneous glycopeptide-intermediate Staphylococ-
cus aureus isolates. Antimicrob Agents Chemother 2014; 58:6668–74. cus aureus related to a device source in an intensive care unit. Infect
13. Banerjee R, Gretes M, Basuino L, Strynadka N, Chambers HF. In vitro Control Hosp Epidemiol 2012; 33:167–74.
selection and characterization of ceftobiprole-resistant methicillin- 33. Gardete S, Tomasz A. Mechanisms of vancomycin resistance in Staph-
resistant Staphylococcus aureus. Antimicrob Agents Chemother 2008; ylococcus aureus. J Clin Invest 2014; 124:2836–40.
52:2089–96. 34. Hafer C, Lin Y, Kornblum J, Lowy FD, Uhlemann AC. Contribution of
14. Hollenbeck BL, Rice LB. Intrinsic and acquired resistance mechanisms selected gene mutations to resistance in clinical isolates of vancomycin-
in enterococcus. Virulence 2012; 3:421–33. intermediate Staphylococcus aureus. Antimicrob Agents Chemother
15. Miller WR, Munita JM, Arias CA. Mechanisms of antibiotic resistance 2012; 56:5845–51.
in enterococci. Expert Rev Anti Infect Ther 2014; 12:1221–36. 35. Mwangi MM, Wu SW, Zhou Y, et al. Tracking the in vivo evolution of
16. Rice LB, Bellais S, Carias LL, et al. Impact of specific pbp5 mutations on multidrug resistance in Staphylococcus aureus by whole-genome se-
expression of beta-lactam resistance in Enterococcus faecium. Antimi- quencing. Proc Natl Acad Sci U S A 2007; 104:9451–6.
crob Agents Chemother 2004; 48:3028–32. 36. Sievert DM, Rudrik JT, Patel JB, McDonald LC, Wilkins MJ, Hageman
17. Galloway-Pena JR, Rice LB, Murray BE. Analysis of PBP5 of early U.S. JC. Vancomycin-resistant Staphylococcus aureus in the United States,
isolates of Enterococcus faecium: sequence variation alone does not ex- 2002–2006. Clin Infect Dis 2008; 46:668–74.
plain increasing ampicillin resistance over time. Antimicrob Agents 37. Rossi F, Diaz L, Wollam A, et al. Transferable vancomycin resistance in a
Chemother 2011; 55:3272–7. community-associated MRSA lineage. N Engl J Med 2014; 370:1524–31.
S56 • CID 2015:61 (Suppl 2) • Munita et al
38. VIBATIV (telavancin) Prescribing Information. Theravance Biopharma 60. Bayer AS, Schneider T, Sahl HG. Mechanisms of daptomycin resistance
Antibiotics, Inc. December 2014. Available at: http://www.vibativ.com. in Staphylococcus aureus: role of the cell membrane and cell wall. Ann N
Accessed 19 March 2015. Y Acad Sci 2013; 1277:139–58.
39. Durata Therapeutics US. Dalvance (dalbavancin for injection), prescrib- 61. Ernst CM, Kuhn S, Slavetinsky CJ, et al. The lipid-modifying multiple
ing information. Available at: http://www.dalvance.com/. Accessed 30 peptide resistance factor is an oligomer consisting of distinct interacting
May 2015. synthase and flippase subunits. MBio 2015; 6:e02340–14.
40. The Medicines Company. Orbactic (oritavancin for injection), prescrib- 62. Yang SJ, Kreiswirth BN, Sakoulas G, et al. Enhanced expression of
ing information. Available at: http://www.orbactiv.com/. Accessed 30 dltABCD is associated with the development of daptomycin nonsus-
March 2015. ceptibility in a clinical endocarditis isolate of Staphylococcus aureus.
41. Zhanel GG, Calic D, Schweizer F, et al. New lipoglycopeptides: a com- J Infect Dis 2009; 200:1916–20.
parative review of dalbavancin, oritavancin and telavancin. Drugs 2010; 63. Peleg AY, Miyakis S, Ward DV, et al. Whole genome characterization of
70:859–86. the mechanisms of daptomycin resistance in clinical and laboratory de-
42. Arias CA, Mendes RE, Stilwell MG, Jones RN, Murray BE. Unmet needs rived isolates of Staphylococcus aureus. PLoS One 2012; 7:e28316.
and prospects for oritavancin in the management of vancomycin-resis- 64. Mehta S, Cuirolo AX, Plata KB, et al. VraSR two-component regulatory
tant enterococcal infections. Clin Infect Dis 2012; 54(suppl 3):S233–8. system contributes to mprF-mediated decreased susceptibility to dapto-
43. Marshall SH, Donskey CJ, Hutton-Thomas R, Salata RA, Rice LB. Gene mycin in in vivo-selected clinical strains of methicillin-resistant Staph-
dosage and linezolid resistance in Enterococcus faecium and Enterococ- ylococcus aureus. Antimicrob Agents Chemother 2012; 56:92–102.
cus faecalis. Antimicrob Agents Chemother 2002; 46:3334–6. 65. Patel JB, Jevitt LA, Hageman J, McDonald LC, Tenover FC. An association
44. Toh SM, Xiong L, Arias CA, et al. Acquisition of a natural resistance between reduced susceptibility to daptomycin and reduced susceptibility to
gene renders a clinical strain of methicillin-resistant Staphylococcus au- vancomycin in Staphylococcus aureus. Clin Infect Dis 2006; 42:1652–3.
reus resistant to the synthetic antibiotic linezolid. Mol Microbiol 2007; 66. Arias CA, Panesso D, McGrath DM, et al. Genetic basis for in vivo dap-
64:1506–14. tomycin resistance in enterococci. N Engl J Med 2011; 365:892–900.
45. Mendes RE, Deshpande LM, Jones RN. Linezolid update: stable in vitro 67. Reyes J, Panesso D, Tran TT, et al. A liaR deletion restores susceptibility
activity following more than a decade of clinical use and summary of to daptomycin and antimicrobial peptides in multidrug-resistant En-
associated resistance mechanisms. Drug Resist Updat 2014; 17:1–12. terococcus faecalis. J Infect Dis 2015; 211:1317–25.
46. Bonilla H, Huband MD, Seidel J, et al. Multicity outbreak of linezolid- 68. Tran TT, Panesso D, Mishra NN, et al. Daptomycin-resistant Enterococ-
resistant Staphylococcus epidermidis associated with clonal spread of a cus faecalis diverts the antibiotic molecule from the division septum and
cfr-containing strain. Clin Infect Dis 2010; 51:796–800. remodels cell membrane phospholipids. MBio 2013; 4:e00281–13.
47. Morales G, Picazo JJ, Baos E, et al. Resistance to linezolid is mediated by 69. Munita JM, Panesso D, Diaz L, et al. Correlation between mutations in
the cfr gene in the first report of an outbreak of linezolid-resistant Staph- liaFSR of Enterococcus faecium and MIC of daptomycin: revisiting dap-
ylococcus aureus. Clin Infect Dis 2010; 50:821–5. tomycin breakpoints. Antimicrob Agents Chemother 2012; 56:4354–9.
48. LaMarre JM, Locke JB, Shaw KJ, Mankin AS. Low fitness cost of the mul- 70. Munita JM, Mishra NN, Alvarez D, et al. Failure of high-dose daptomy-
tidrug resistance gene cfr. Antimicrob Agents Chemother 2011; 55:3714–9. cin for bacteremia caused by daptomycin-susceptible Enterococcus fae-
49. Diaz L, Kontoyiannis DP, Panesso D, et al. Dissecting the mechanisms cium harboring LiaSR substitutions. Clin Infect Dis 2014; 59:1277–80.
of linezolid resistance in a Drosophila melanogaster infection model of 71. Garcia-de-la-Maria C, Pericas JM, Del Rio A, et al; Hospital Clinic Ex-
Staphylococcus aureus. J Infect Dis 2013; 208:83–91. perimental Endocarditis Study Group. Early in vitro and in vivo devel-
50. Locke JB, Zurenko GE, Shaw KJ, Bartizal K. Tedizolid for the manage- opment of high-level daptomycin resistance is common in mitis group
ment of human infections: in vitro characteristics. Clin Infect Dis 2014; streptococci after exposure to daptomycin. Antimicrob Agents Chemo-
58(suppl 1):S35–42. ther 2013; 57:2319–25.
51. Baos E, Candel FJ, Merino P, Pena I, Picazo JJ. Characterization and 72. Akins RL, Katz BD, Monahan C, Alexander D. Characterization of
monitoring of linezolid-resistant clinical isolates of Staphylococcus epi- high-level daptomycin resistance in viridans group streptococci devel-
dermidis in an intensive care unit 4 years after an outbreak of infection oped upon in vitro exposure to daptomycin. Antimicrob Agents Che-
by cfr-mediated linezolid-resistant Staphylococcus aureus. Diagn Micro- mother 2015; 59:2102–12.
biol Infect Dis 2013; 76:325–9. 73. Yang SJ, Xiong YQ, Boyle-Vavra S, Daum R, Jones T, Bayer AS. Dapto-
52. Locke JB, Hilgers M, Shaw KJ. Novel ribosomal mutations in Staphylococcus mycin-oxacillin combinations in treatment of experimental endocardi-
aureus strains identified through selection with the oxazolidinones linezolid tis caused by daptomycin-nonsusceptible strains of methicillin-resistant
and torezolid (TR-700). Antimicrob Agents Chemother 2009; 53:5265–74. Staphylococcus aureus with evolving oxacillin susceptibility (the “seesaw
53. Mendes RE, Hogan PA, Streit JM, Jones RN, Flamm RK. Zyvox® Annual effect”). Antimicrob Agents Chemother 2010; 54:3161–9.
Appraisal of Potency and Spectrum (ZAAPS) program: report of linezolid 74. Sakoulas G, Bayer AS, Pogliano J, et al. Ampicillin enhances daptomy-
activity over 9 years (2004–12). J Antimicrob Chemother 2014; 69:1582–8. cin- and cationic host defense peptide-mediated killing of ampicillin-
54. Diaz L, Kiratisin P, Mendes RE, Panesso D, Singh KV, Arias CA. Trans- and vancomycin-resistant Enterococcus faecium. Antimicrob Agents
ferable plasmid-mediated resistance to linezolid due to cfr in a human Chemother 2012; 56:838–44.
clinical isolate of Enterococcus faecalis. Antimicrob Agents Chemother 75. Dhand A, Bayer AS, Pogliano J, et al. Use of antistaphylococcal beta-
2012; 56:3917–22. lactams to increase daptomycin activity in eradicating persistent bacter-
55. Wang Y, Li D, Song L, et al. First report of the multiresistance gene cfr in emia due to methicillin-resistant Staphylococcus aureus: role of
Streptococcus suis. Antimicrob Agents Chemother 2013; 57:4061–3. enhanced daptomycin binding. Clin Infect Dis 2011; 53:158–63.
56. Pogliano J, Pogliano N, Silverman JA. Daptomycin-mediated reorgani- 76. Sakoulas G, Rose W, Nonejuie P, et al. Ceftaroline restores daptomycin
zation of membrane architecture causes mislocalization of essential cell activity against daptomycin-nonsusceptible vancomycin-resistant En-
division proteins. J Bacteriol 2012; 194:4494–504. terococcus faecium. Antimicrob Agents Chemother 2014; 58:1494–500.
57. Muraih JK, Pearson A, Silverman J, Palmer M. Oligomerization of dap- 77. Berti AD, Sakoulas G, Nizet V, Tewhey R, Rose WE. Beta-lactam anti-
tomycin on membranes. Biochim Biophys Acta 2011; 1808:1154–60. biotics targeting PBP1 selectively enhance daptomycin activity against
58. Fowler VG Jr., Boucher HW, Corey GR, et al. Daptomycin versus stan- methicillin-resistant Staphylococcus aureus. Antimicrob Agents Che-
dard therapy for bacteremia and endocarditis caused by Staphylococcus mother 2013; 57:5005–12.
aureus. N Engl J Med 2006; 355:653–65. 78. Diaz L, Tran TT, Munita JM, et al. Whole-genome analyses of Entero-
59. Humphries RM, Pollett S, Sakoulas G. A current perspective on daptomy- coccus faecium isolates with diverse daptomycin MICs. Antimicrob
cin for the clinical microbiologist. Clin Microbiol Rev 2013; 26:759–80. Agents Chemother 2014; 58:4527–34.
Gram-positive Resistance • CID 2015:61 (Suppl 2) • S57
You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 2007 AP Statistics Multiple Choice ExamDocument17 pages2007 AP Statistics Multiple Choice ExamJalaj SoodNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Drew Marine Chemical ManualDocument36 pagesDrew Marine Chemical ManualcpiquiNo ratings yet
- Primary Health Care: Mr. John Michael M. Pitoy, B.S.N., R.NDocument44 pagesPrimary Health Care: Mr. John Michael M. Pitoy, B.S.N., R.NJohn Michael Manlupig Pitoy100% (9)
- Module-1-ISO 13485-DocumentDocument7 pagesModule-1-ISO 13485-Documentsri manthNo ratings yet
- SinusitisDocument402 pagesSinusitisIsidro Roberto Santana Gonzalez100% (1)
- Enterococo Faecium Vanco Resistente 2017 PDFDocument12 pagesEnterococo Faecium Vanco Resistente 2017 PDFGustavo UrriagoNo ratings yet
- Waves of ResistenceDocument31 pagesWaves of ResistencemotibaNo ratings yet
- MIC Creep Vancomicina PDFDocument4 pagesMIC Creep Vancomicina PDFGustavo UrriagoNo ratings yet
- Clinical Practice Guidelines by The Infectious DiseasesDocument38 pagesClinical Practice Guidelines by The Infectious DiseasesMuhammad FajriNo ratings yet
- hVISA Sin Expocision A Vancomicina PDFDocument6 pageshVISA Sin Expocision A Vancomicina PDFGustavo UrriagoNo ratings yet
- Cefazolina Vs Naficilina Oxacilina para SAMS 2017 PDFDocument25 pagesCefazolina Vs Naficilina Oxacilina para SAMS 2017 PDFGustavo UrriagoNo ratings yet
- hVISa y VISA 2007 PDFDocument9 pageshVISa y VISA 2007 PDFGustavo UrriagoNo ratings yet
- hVISA 2015 PDFDocument4 pageshVISA 2015 PDFGustavo UrriagoNo ratings yet
- BORSA Problema Mas Comun Del Esperado 2017 PDFDocument7 pagesBORSA Problema Mas Comun Del Esperado 2017 PDFGustavo UrriagoNo ratings yet
- Enterococo Resistente PDFDocument8 pagesEnterococo Resistente PDFGustavo UrriagoNo ratings yet
- Cefazolin o Nafcilin Vs Vancomicina PDFDocument7 pagesCefazolin o Nafcilin Vs Vancomicina PDFGustavo UrriagoNo ratings yet
- Betalactamicos Vs Vancomicina para SAMS PDFDocument7 pagesBetalactamicos Vs Vancomicina para SAMS PDFGustavo UrriagoNo ratings yet
- Clinical Practice Guidelines by The Infectious DiseasesDocument38 pagesClinical Practice Guidelines by The Infectious DiseasesMuhammad FajriNo ratings yet
- 100518-Concrete Roof Installation Manual 0515Document26 pages100518-Concrete Roof Installation Manual 0515Moe Oo HtunNo ratings yet
- Synergic Antiobesity Effects of Bitter Melon Water Extract and Platycodin-D in Genetically Obese MiceDocument9 pagesSynergic Antiobesity Effects of Bitter Melon Water Extract and Platycodin-D in Genetically Obese Micegege wpNo ratings yet
- Leon County Sheriff'S Office Daily Booking Report 18-Oct-2020 Page 1 of 3Document3 pagesLeon County Sheriff'S Office Daily Booking Report 18-Oct-2020 Page 1 of 3WCTV Digital TeamNo ratings yet
- شيتات محطات كهربية PDFDocument8 pagesشيتات محطات كهربية PDFhazem saeidNo ratings yet
- Gazettes 1686290048232Document2 pagesGazettes 1686290048232allumuraliNo ratings yet
- Cleaning Disinfecting School ClassroomsDocument2 pagesCleaning Disinfecting School ClassroomsFitz JaminitNo ratings yet
- Calcium Cyanide: Hydrogen Cyanide. CONSULT THE NEW JERSEYDocument6 pagesCalcium Cyanide: Hydrogen Cyanide. CONSULT THE NEW JERSEYbacabacabacaNo ratings yet
- Nutrients: Dietary Fiber, Atherosclerosis, and Cardiovascular DiseaseDocument11 pagesNutrients: Dietary Fiber, Atherosclerosis, and Cardiovascular Diseasemichael palitNo ratings yet
- Exercises: (A) Read The Following PassageDocument2 pagesExercises: (A) Read The Following PassageNur Nezanna0% (1)
- C783 - Intake Manifold 1 Temperature-Abnormal Rate of ChangeDocument4 pagesC783 - Intake Manifold 1 Temperature-Abnormal Rate of ChangeLucas CamposNo ratings yet
- The Safe Motherhood InitiativeDocument3 pagesThe Safe Motherhood InitiativeAnonymous g6L7jJWNo ratings yet
- Components of FitnessDocument3 pagesComponents of Fitnessapi-3830277100% (1)
- Sandwich StoichiometryDocument2 pagesSandwich StoichiometryMaysaa El HarakehNo ratings yet
- 'Last Season's Man'Document7 pages'Last Season's Man'Bishal Kumar SahuNo ratings yet
- Natural Resources NotesDocument5 pagesNatural Resources NotesRajesh Kumar GuptaNo ratings yet
- Tended Range Sixteen Channel Supervised Stationary ReceiverDocument2 pagesTended Range Sixteen Channel Supervised Stationary ReceiverAimee chaconNo ratings yet
- Material Safety Data Sheet Glyphosate 5.4Document5 pagesMaterial Safety Data Sheet Glyphosate 5.4Ahfi Rizqi FajrinNo ratings yet
- Techno LabDocument3 pagesTechno LabA M FaisalNo ratings yet
- Cocoa Nursery Manual Feb 2013Document51 pagesCocoa Nursery Manual Feb 2013jeffreyNo ratings yet
- Client Travel Policy Guidelines Nunavut Health Care PlanDocument8 pagesClient Travel Policy Guidelines Nunavut Health Care PlanNunatsiaqNewsNo ratings yet
- Barista Coffee Company LTDDocument3 pagesBarista Coffee Company LTDGanesh AnandNo ratings yet
- 138 Student Living: New Returning Yes NoDocument2 pages138 Student Living: New Returning Yes NojevaireNo ratings yet
- The Company - MicroDocument2 pagesThe Company - MicroMai Hương QuỳnhNo ratings yet
- Issues Pertaining To Maintenance of WifeDocument2 pagesIssues Pertaining To Maintenance of WifeVaishnavi YadavNo ratings yet
- 1.indentify The Functions of Various Keys On The Key BoardDocument83 pages1.indentify The Functions of Various Keys On The Key BoardMuhammad AbbasNo ratings yet