You might also like
- OB-GYN - Shelf Review NotesDocument47 pagesOB-GYN - Shelf Review NotesJackJoseph95% (19)
- UVA Family Medicine Qbank Answers PDFDocument101 pagesUVA Family Medicine Qbank Answers PDFjamesmgang100% (1)
- Study Guide For OBGYNDocument34 pagesStudy Guide For OBGYNFiorellaBeatriz100% (1)
- Comat NotesDocument33 pagesComat NotesVee Mend100% (1)
- Moon Time: Harness The Energy of Your Menstrual Cycle by Lucy H. Pearce (Sample) Womancraft PublishingDocument29 pagesMoon Time: Harness The Energy of Your Menstrual Cycle by Lucy H. Pearce (Sample) Womancraft PublishingWomancraft Publishing50% (4)
- Dr. Pestana's Surgery Notes: Pocket-Sized Review for the Surgical Clerkship and Shelf ExamsFrom EverandDr. Pestana's Surgery Notes: Pocket-Sized Review for the Surgical Clerkship and Shelf ExamsRating: 5 out of 5 stars5/5 (1)
- Step 2 CK - NBME 7 Answers UncompleteDocument16 pagesStep 2 CK - NBME 7 Answers UncompleteDuke83% (12)
- High-Yield Shelf NotesDocument170 pagesHigh-Yield Shelf Notes1nertia100% (10)
- OB GYN Shelf Review Notes PDFDocument47 pagesOB GYN Shelf Review Notes PDFAnnaNo ratings yet
- Step 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionFrom EverandStep 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionNo ratings yet
- Ob Gyn Notes - UWorld 2018Document17 pagesOb Gyn Notes - UWorld 2018Fake person0% (1)
- CMS Ob&Gyn 4 AnswersDocument21 pagesCMS Ob&Gyn 4 AnswersVictor Conan100% (2)
- High Yield Surgery Notes PDFDocument39 pagesHigh Yield Surgery Notes PDFrom92100% (1)
- Family Medicine Shelf ReviewDocument69 pagesFamily Medicine Shelf ReviewnomansnNo ratings yet
- Endometrial CA and Pregnancy Risk FactorsDocument11 pagesEndometrial CA and Pregnancy Risk FactorsLaura Lopez Roca0% (1)
- Emergency Head, Chest, Abdominal and Orthopedic Trauma ReviewDocument8 pagesEmergency Head, Chest, Abdominal and Orthopedic Trauma ReviewJayson Marwaha100% (2)
- CMS Peads 1 & 2 AnswersDocument12 pagesCMS Peads 1 & 2 AnswersMohamed Abib100% (1)
- Nbme Obgyn Searchable AnsweredDocument50 pagesNbme Obgyn Searchable Answeredexplore100% (8)
- OBgyn ShelfDocument10 pagesOBgyn ShelfHassan R. G.100% (1)
- IM STEP 2 NotesDocument74 pagesIM STEP 2 Notesyanks1120100% (3)
- HY PediatricsDocument56 pagesHY PediatricsJamesIwuNo ratings yet
- MAIN Divine Intervention Step 2CK Podcasts Notes - Read OnlyDocument829 pagesMAIN Divine Intervention Step 2CK Podcasts Notes - Read OnlyJonathan Mariano100% (2)
- OBGYN Shelf SR: Top 40 OBGYN Questions & AnswersDocument13 pagesOBGYN Shelf SR: Top 40 OBGYN Questions & AnswerslindaNo ratings yet
- APGODocument49 pagesAPGOiamdonutNo ratings yet
- Family Medicine Shelf Review: Vaccination and Screening GuidelinesDocument142 pagesFamily Medicine Shelf Review: Vaccination and Screening GuidelinesAnonymous kOPWA2s0% (1)
- Doctor High Yield Obgyn - Not AnnotatedDocument34 pagesDoctor High Yield Obgyn - Not AnnotatedEmanuella Gomez100% (2)
- EMMaA - IMDocument100 pagesEMMaA - IMR IghtzedNo ratings yet
- Step 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionFrom EverandStep 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionNo ratings yet
- Pediatrics SHELFDocument31 pagesPediatrics SHELFAztec100% (5)
- NBME Family Medicine Form 1 Answers & ExplanationsDocument8 pagesNBME Family Medicine Form 1 Answers & ExplanationsAnna100% (1)
- Peds Shelf NotesDocument74 pagesPeds Shelf NotesRandy BornmannNo ratings yet
- Surgery Nbme ReviewDocument3 pagesSurgery Nbme Reviewhannahylee71188% (8)
- HY PediatricsDocument57 pagesHY PediatricsJennifer Ross-ComptisNo ratings yet
- Obgyn UWISE Notes (And Master The Boards)Document8 pagesObgyn UWISE Notes (And Master The Boards)Laura Lopez Roca100% (5)
- Mehlmanmedical Hy ObgynDocument30 pagesMehlmanmedical Hy ObgynJennifer Ross-Comptis100% (1)
- Divine Intervention Episode 24 Surgery Shelf ReviewDocument118 pagesDivine Intervention Episode 24 Surgery Shelf ReviewPedro Weslley100% (3)
- The Electrical Patterns of Life - The Work of Dr. Harold SDocument4 pagesThe Electrical Patterns of Life - The Work of Dr. Harold SSilvio ArévalosNo ratings yet
- Gordon's Functional Health AssessmentDocument11 pagesGordon's Functional Health AssessmentRaquel M. Mendoza100% (1)
- NBME OBGYN2 6 Wrong With Answers SearchableDocument50 pagesNBME OBGYN2 6 Wrong With Answers Searchabledramcdover96% (26)
- Nbme Medicine Shelf Review Session 2Document142 pagesNbme Medicine Shelf Review Session 2Swisskelly1100% (1)
- Divine Intervention Episode 21 Peds Shelf Review PDFDocument139 pagesDivine Intervention Episode 21 Peds Shelf Review PDFSwisskelly1No ratings yet
- International Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessFrom EverandInternational Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessRaghav GovindarajanNo ratings yet
- Uwise HYDocument3 pagesUwise HYJack GuccioneNo ratings yet
- NBME Medicine Shelf Review Session 1 High-Yield TopicsDocument54 pagesNBME Medicine Shelf Review Session 1 High-Yield TopicsHersheyth AggarwalNo ratings yet
- Jeff Pages - Homeopathic SymptomsDocument8 pagesJeff Pages - Homeopathic SymptomsSatish MishraNo ratings yet
- HY PsychDocument19 pagesHY PsychJamesIwuNo ratings yet
- Family Medicine Review NotesDocument6 pagesFamily Medicine Review NotesmojdaNo ratings yet
- Peds NBME QuestionsDocument14 pagesPeds NBME QuestionsAbrar Khan100% (7)
- Peds Shelf NotesDocument9 pagesPeds Shelf NotesclaravhvuNo ratings yet
- OBGYN Shelf NotesDocument7 pagesOBGYN Shelf NotesaelteeNo ratings yet
- Comprehensive medical case review with diagnoses and management optionsDocument1 pageComprehensive medical case review with diagnoses and management optionsVikasYellapu89% (18)
- The Development of A MenstrualDocument15 pagesThe Development of A MenstrualralukadkNo ratings yet
- Vademecum Fitoterapia Tradicional Chinesa (Pedro Choy)Document222 pagesVademecum Fitoterapia Tradicional Chinesa (Pedro Choy)jjseguin100% (4)
- L T College of Nursing SNDT University Churchgate Lesson Plan On Nursing Care of A Patient With Menstrual DisordersDocument13 pagesL T College of Nursing SNDT University Churchgate Lesson Plan On Nursing Care of A Patient With Menstrual DisordersPriyanka NilewarNo ratings yet
- Mehlmanmedical Hy Surgery Part IDocument20 pagesMehlmanmedical Hy Surgery Part IJennifer Ross-Comptis100% (1)
- Clinical Pearls for Reproductive HealthDocument4 pagesClinical Pearls for Reproductive HealthD50% (4)
- OB/GynDocument11 pagesOB/GynAnonymous TYyF7Ul9o100% (2)
- Pediatrics Shelf TopicsDocument5 pagesPediatrics Shelf TopicsSam Zeez100% (2)
- OBGYN Form 3 Answers KeyDocument2 pagesOBGYN Form 3 Answers KeyGrace0% (1)
- DIVISION LEVEL POPQUIZ 2023-cDocument13 pagesDIVISION LEVEL POPQUIZ 2023-cfatimabusaco7100% (1)
- David P. Barash-Homo Mysterious - Evolutionary Puzzles of Human Nature-Oxford University Press, USA (2012) PDFDocument340 pagesDavid P. Barash-Homo Mysterious - Evolutionary Puzzles of Human Nature-Oxford University Press, USA (2012) PDFalphanco100% (1)
- Beneficial SummaryDocument54 pagesBeneficial Summaryimamrassisociety100% (2)
- SURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 1From EverandSURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 1Rating: 5 out of 5 stars5/5 (2)
- How To Pass MRCPDocument2 pagesHow To Pass MRCPdooja10100% (2)
- Shelf High Yield Hit ParadeDocument3 pagesShelf High Yield Hit ParadeAakash ShahNo ratings yet
- Family MedicineDocument3 pagesFamily MedicineScott YeeNo ratings yet
- Vaginal Bleeding in PregnancyDocument4 pagesVaginal Bleeding in PregnancyAra BaltarNo ratings yet
- Cancer Epigenetics New Therapies and New Challenges REVIEW ARTICLEDocument25 pagesCancer Epigenetics New Therapies and New Challenges REVIEW ARTICLEece142No ratings yet
- BAP Guidelines PerinatalDocument34 pagesBAP Guidelines Perinatalrocsa11No ratings yet
- Cancer Epigenetics New Therapies and New Challenges REVIEW ARTICLEDocument9 pagesCancer Epigenetics New Therapies and New Challenges REVIEW ARTICLEece142No ratings yet
- Alternative Certificate of Foundation Competence - 2018Document12 pagesAlternative Certificate of Foundation Competence - 2018Chris RaduNo ratings yet
- Alternative Certificate of Foundation Competence 2018 Reference GuideDocument12 pagesAlternative Certificate of Foundation Competence 2018 Reference Guideece142No ratings yet
- Big Data Approaches To Decomposing Heterogeneity Across The Autism SpectrumDocument30 pagesBig Data Approaches To Decomposing Heterogeneity Across The Autism Spectrumece142No ratings yet
- Croft LeafletDocument2 pagesCroft Leafletece142No ratings yet
- Alternative Certificate of Foundation Competence 2018 Reference GuideDocument12 pagesAlternative Certificate of Foundation Competence 2018 Reference Guideece142No ratings yet
- Mehler2015 Article TreatmentsOfMedicalComplicatioDocument72 pagesMehler2015 Article TreatmentsOfMedicalComplicatioece142No ratings yet
- Online Ticket Refund FormDocument1 pageOnline Ticket Refund Formece142No ratings yet
- Evidence of Foundation Competence Applicant Guide 2018Document6 pagesEvidence of Foundation Competence Applicant Guide 2018ece142No ratings yet
- 1745 6215 12 175Document13 pages1745 6215 12 175ece142No ratings yet
- Acute Support Allied Health Clinical PrioritisationDocument4 pagesAcute Support Allied Health Clinical Prioritisationece142No ratings yet
- Evidence of Foundation Competence Signatory Guide 2018Document4 pagesEvidence of Foundation Competence Signatory Guide 2018ece142No ratings yet
- JD Approval ProcessDocument2 pagesJD Approval Processece142No ratings yet
- Acute Support Allied Health Clinical PrioritisationDocument4 pagesAcute Support Allied Health Clinical Prioritisationece142No ratings yet
- Clinical Characteristics Associated With The Prescribing of SSRI Medication in Adolescents With Major Unipolar..Document12 pagesClinical Characteristics Associated With The Prescribing of SSRI Medication in Adolescents With Major Unipolar..ece142No ratings yet
- Mehler2015 Article TreatmentsOfMedicalComplicatio PDFDocument7 pagesMehler2015 Article TreatmentsOfMedicalComplicatio PDFece142No ratings yet
- V 031 P 00582Document5 pagesV 031 P 00582ece142No ratings yet
- Mehler2015 Article TreatmentsOfMedicalComplicatio PDFDocument7 pagesMehler2015 Article TreatmentsOfMedicalComplicatio PDFece142No ratings yet
- WAST 2018 Person Specification June 18Document3 pagesWAST 2018 Person Specification June 18ece142No ratings yet
- FP Reference Guide - Key Changes For 2017-1Document2 pagesFP Reference Guide - Key Changes For 2017-1ece142No ratings yet
- BAP Guidelines PerinatalDocument3 pagesBAP Guidelines Perinatalece142No ratings yet
- Bulimia Nervosa - Medical Complications: Review Open AccessDocument5 pagesBulimia Nervosa - Medical Complications: Review Open Accessece142No ratings yet
- Umj7603 177cDocument1 pageUmj7603 177cece142No ratings yet
- Book Reviews: Get Through Mrcophth Part 3: EmqsDocument2 pagesBook Reviews: Get Through Mrcophth Part 3: Emqsece142No ratings yet
- BAP Guidelines PerinatalDocument34 pagesBAP Guidelines Perinatalrocsa11No ratings yet
- Identification of Disease GenesDocument24 pagesIdentification of Disease Genesece142No ratings yet
- Miyagawa Et Al-2015-Human Genome VariationDocument4 pagesMiyagawa Et Al-2015-Human Genome Variationece142No ratings yet
- Gynae ClinDocument10 pagesGynae ClinUmut KNo ratings yet
- iTIJ:: P4Yicai. Etfal - Uati OnDocument4 pagesiTIJ:: P4Yicai. Etfal - Uati OnBartolome MercadoNo ratings yet
- Assessment Scales For Sexual Disorders: A Review: Sandeep Grover and Anish ShouanDocument18 pagesAssessment Scales For Sexual Disorders: A Review: Sandeep Grover and Anish ShouanTantonio Tri PutraNo ratings yet
- Legal MedicineDocument8 pagesLegal MedicineValredNo ratings yet
- Abnormal Uterine Bleeding in The Adolescent CME 2020Document7 pagesAbnormal Uterine Bleeding in The Adolescent CME 2020Mariana HernandezNo ratings yet
- Si ProjectDocument51 pagesSi ProjectRohit singhNo ratings yet
- Medical History QuestionnaireDocument3 pagesMedical History QuestionnaireDre EzNo ratings yet
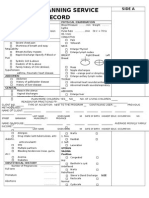
- Family Planning Service RecordDocument3 pagesFamily Planning Service RecordRJay Mon Marcos100% (2)
- Management of Asherman's SyndromeDocument14 pagesManagement of Asherman's SyndromeEquipmed VenezuelaNo ratings yet
- Saranya Wattanakumtornkul, MDDocument46 pagesSaranya Wattanakumtornkul, MDPattanop NgaodulyawatNo ratings yet
- Caffeine Intake and Menstrual CyclesDocument8 pagesCaffeine Intake and Menstrual CyclesBelle Denniese FontelarNo ratings yet
- Gynecology 2020 Copy 2Document620 pagesGynecology 2020 Copy 2school adressNo ratings yet
- Fek 1Document13 pagesFek 1school adressNo ratings yet
- Mirena BrochureDocument24 pagesMirena BrochureNamrata HarishNo ratings yet
- Mock Exam 2Document18 pagesMock Exam 2Anna StacyNo ratings yet
- Mullerian Duct Abnormalities, Hirsutism, Bacterial Vaginosis & IUCDsDocument4 pagesMullerian Duct Abnormalities, Hirsutism, Bacterial Vaginosis & IUCDsrohitNo ratings yet
- Atreyee Gupta - Yishu Journal of Contemporary Chinese Art PDFDocument10 pagesAtreyee Gupta - Yishu Journal of Contemporary Chinese Art PDFAtreyee GuptaNo ratings yet
- Antepartal CareDocument9 pagesAntepartal CareChristopher R. Bañez-Full Account100% (1)
- Diane 35 PM pt3 PDFDocument11 pagesDiane 35 PM pt3 PDFHum BlumNo ratings yet
- Evaluate The Effectiveness of Structured Teaching Program Regarding Menopausal Syndrome Among The Peri Menopausal Women in Bandarulanka, Amalapuram, Andhra PradeshDocument9 pagesEvaluate The Effectiveness of Structured Teaching Program Regarding Menopausal Syndrome Among The Peri Menopausal Women in Bandarulanka, Amalapuram, Andhra PradeshInternational Journal of Innovative Science and Research TechnologyNo ratings yet