You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- CFLGA Handbook - Section On Assessment CriteriaDocument25 pagesCFLGA Handbook - Section On Assessment CriteriaJim100% (6)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Shoulder ExaminationDocument4 pagesShoulder ExaminationYS NateNo ratings yet
- Kanker ServiksDocument308 pagesKanker ServiksponekNo ratings yet
- Checklist Dmpa EnglishDocument3 pagesChecklist Dmpa EnglishponekNo ratings yet
- Sadiq KhanDocument5 pagesSadiq KhanponekNo ratings yet
- Scientific Schedule: Alarm Course Day 1Document11 pagesScientific Schedule: Alarm Course Day 1ponekNo ratings yet
- Preclinical Condition MagementDocument27 pagesPreclinical Condition MagementponekNo ratings yet
- Analisis Pengendalian Alkes Farmasi Di Rs Pangkal PinangDocument12 pagesAnalisis Pengendalian Alkes Farmasi Di Rs Pangkal PinangponekNo ratings yet
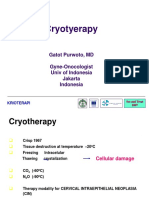
- CRYOTERAPI See&Treat GatotDocument20 pagesCRYOTERAPI See&Treat GatotponekNo ratings yet
- Research Penis EnlargementDocument10 pagesResearch Penis Enlargementalan100% (1)
- Lumenis Novus Varia Indications For Use As Requested by FdaDocument8 pagesLumenis Novus Varia Indications For Use As Requested by FdaM.r SadrshiraziNo ratings yet
- Sponge Count Has Been and Still Is One of The Most Important Responsibilities of An Operating Room NurseDocument3 pagesSponge Count Has Been and Still Is One of The Most Important Responsibilities of An Operating Room NurseSiena Lou CeniaNo ratings yet
- NbeDocument37 pagesNbesenthiljayanthiNo ratings yet
- Tools and Techniques To Reduce Pain During Labor To Have A Natural BirthDocument18 pagesTools and Techniques To Reduce Pain During Labor To Have A Natural BirthAbir Gasmi100% (2)
- What Is An Ibclc Flyer IlcaDocument2 pagesWhat Is An Ibclc Flyer Ilcaapi-275110874No ratings yet
- Rajiv Gandhi University Thesis Topics in OphthalmologyDocument6 pagesRajiv Gandhi University Thesis Topics in Ophthalmologygyuusthig100% (1)
- Gynecologic Neoplasia: Vagina: Dr. Maria Cristina S. Estella - SantosDocument4 pagesGynecologic Neoplasia: Vagina: Dr. Maria Cristina S. Estella - SantosMaikka IlaganNo ratings yet
- TabeDocument6 pagesTabeRhod Bernaldez EstaNo ratings yet
- Resume-Preetha JoseDocument7 pagesResume-Preetha Joseapi-551188095No ratings yet
- Kegawatdaruratan Otak (Siloam - 14 Mei 2008)Document34 pagesKegawatdaruratan Otak (Siloam - 14 Mei 2008)Ruki HartawanNo ratings yet
- 20844Document119 pages20844Mark ReinhardtNo ratings yet
- NCM 102 PDFDocument8 pagesNCM 102 PDFjnnfrleeeNo ratings yet
- Committee Report Brgy Ordinance - For ScribdDocument2 pagesCommittee Report Brgy Ordinance - For ScribdJoshelle B. Bancilo100% (3)
- Gilmore v. Fulbright & Jaworski, LLP - Document No. 14Document21 pagesGilmore v. Fulbright & Jaworski, LLP - Document No. 14Justia.comNo ratings yet
- AmenorrheaDocument41 pagesAmenorrheadoraNo ratings yet
- Male Reproductive SystemDocument49 pagesMale Reproductive SystemRinkish Dalliah50% (2)
- Multiple Pregnancy PDFDocument12 pagesMultiple Pregnancy PDFHaidar AmrNo ratings yet
- Module Competence Based 02.09.2019Document36 pagesModule Competence Based 02.09.2019goutham kankanamNo ratings yet
- BHEL Doctors - Mobile Number and Email IdDocument4 pagesBHEL Doctors - Mobile Number and Email IdPravesh Sethi100% (1)
- Saluyot Leaves As Acoustic Gel For Ultrasound ImagingDocument5 pagesSaluyot Leaves As Acoustic Gel For Ultrasound ImagingZERI LABADIANo ratings yet
- Chapter 3 Admission (Hospital Organization)Document5 pagesChapter 3 Admission (Hospital Organization)Reshiram KyuramNo ratings yet
- Summary of Purposes and ObjectivesDocument19 pagesSummary of Purposes and Objectivesrodolfo opido100% (1)
- Ijpo 5 3 429 434Document7 pagesIjpo 5 3 429 434Shahid HussainNo ratings yet
- Pa0043 Sub Christine+david Harmes PDFDocument8 pagesPa0043 Sub Christine+david Harmes PDFTheNewChildrensHospitalNo ratings yet
- CholecystitisDocument15 pagesCholecystitisHala LeeNo ratings yet
- Mendelson Syndrome - StatPearls - NCBI BookshelfDocument8 pagesMendelson Syndrome - StatPearls - NCBI Bookshelfcesar aNo ratings yet
- Experienced Nys Massage Therapist Betsy LenkeDocument1 pageExperienced Nys Massage Therapist Betsy Lenkeapi-240088553No ratings yet