You might also like
- Pain Neuroscience EducationDocument26 pagesPain Neuroscience EducationGustavo Cabanas100% (1)
- Cns 765 Final Case StudyDocument10 pagesCns 765 Final Case Studyapi-581708536No ratings yet
- Autonomic Dysreflexia Treatment AlgorithmDocument1 pageAutonomic Dysreflexia Treatment AlgorithmdandrewmNo ratings yet
- MCQ1FULLDocument176 pagesMCQ1FULLtheintrov100% (11)
- Empirical Antimicrobial Therapy Prescribing Guidance For AdultsDocument1 pageEmpirical Antimicrobial Therapy Prescribing Guidance For AdultsPsychology TodayNo ratings yet
- Pediatric Bradycardia With A Pulse and Poor Perfusion AlgorithmDocument1 pagePediatric Bradycardia With A Pulse and Poor Perfusion AlgorithmRadhiatul MardhiahNo ratings yet
- Acute Coronary Syndromes Algorithm: Patient Has Signs Suggestive of Ischemia or InfarctionDocument1 pageAcute Coronary Syndromes Algorithm: Patient Has Signs Suggestive of Ischemia or Infarctionjohndoe1995No ratings yet
- Treatment Algorithm For Autonomic Dysreflexia (Hypertensive Crisis) in Spinal Cord InjuryDocument1 pageTreatment Algorithm For Autonomic Dysreflexia (Hypertensive Crisis) in Spinal Cord InjuryHAYME THARRISNo ratings yet
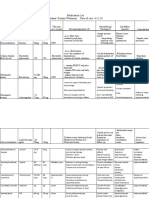
- Nursing responsibilities for common drugsDocument3 pagesNursing responsibilities for common drugsVinssy RevicNo ratings yet
- Tachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDocument1 pageTachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDendy Frannuzul RamadhanNo ratings yet
- AlgorithmACLStachycardiawithapulse PDFDocument1 pageAlgorithmACLStachycardiawithapulse PDFDendy Frannuzul RamadhanNo ratings yet
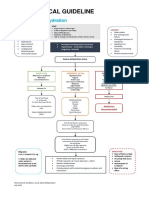
- AdultDehydrationGuidelineJuly2015 PDFDocument3 pagesAdultDehydrationGuidelineJuly2015 PDFmarselamgeNo ratings yet
- TRANSF Sangre MapaDocument1 pageTRANSF Sangre MapaSiu Lin WongNo ratings yet
- ACLS 2020 Algorithms: American Heart Association 2020 GuidelinesDocument8 pagesACLS 2020 Algorithms: American Heart Association 2020 GuidelinesNofi Nurina100% (4)
- Captopril Is An ACE Inhibitor and Works by Relaxing Blood Vessels So That Blood Can Flow More EasilyDocument4 pagesCaptopril Is An ACE Inhibitor and Works by Relaxing Blood Vessels So That Blood Can Flow More EasilyKsksksksNo ratings yet
- Adult Dehydration Guideline Final 2015Document3 pagesAdult Dehydration Guideline Final 2015Brillyant S RaintamaNo ratings yet
- Nicardipine Mechanism of Action, Indications, Side Effects and Nursing ResponsibilitiesDocument3 pagesNicardipine Mechanism of Action, Indications, Side Effects and Nursing ResponsibilitiesQueenzee AsuncionNo ratings yet
- Asystole/PEA: Epinephrine 0.1 ML/KG ASAPDocument1 pageAsystole/PEA: Epinephrine 0.1 ML/KG ASAPAlejandro MusaNo ratings yet
- Week 3 HospDocument2 pagesWeek 3 Hospapi-507319784No ratings yet
- Algoritma Ambulance - PHCDocument11 pagesAlgoritma Ambulance - PHCYassarNo ratings yet
- Emergency Drugs: Drug Action Indications Adverse Effects Contraindications Nursing Management Atropine SulfateDocument15 pagesEmergency Drugs: Drug Action Indications Adverse Effects Contraindications Nursing Management Atropine Sulfate092109No ratings yet
- Nameof DrugDocument16 pagesNameof DrugshiNo ratings yet
- Sevoflurane 2Document2 pagesSevoflurane 2Tasha_Caballer_379No ratings yet
- Emergency MedsDocument12 pagesEmergency MedsAnne Ruth OlinNo ratings yet
- ACS Algorithm 2016 PDFDocument1 pageACS Algorithm 2016 PDFrabin1994No ratings yet
- Cardiac drugs guide for nursing managementDocument4 pagesCardiac drugs guide for nursing managementanne_18No ratings yet
- ToxicosisDocument1 pageToxicosisAnaNo ratings yet
- Critical Care Drug Reference SheetDocument12 pagesCritical Care Drug Reference SheetYanina CoxNo ratings yet
- Dabe Drug StudyDocument3 pagesDabe Drug StudyMary Joy Anne LucasNo ratings yet
- Emergecy DrugsDocument6 pagesEmergecy DrugsChristopher EsguerraNo ratings yet
- Fluphenazine Drug Study - DoxDocument3 pagesFluphenazine Drug Study - Doxan naNo ratings yet
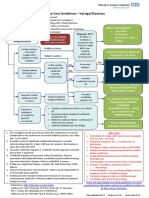
- Primary Care Guidelines VertigoDocument1 pagePrimary Care Guidelines VertigoSyahidatul Kautsar NajibNo ratings yet
- DS Male SurgicalDocument6 pagesDS Male SurgicalErryl Justine AdvinculaNo ratings yet
- Drug Study Case AnalysisDocument7 pagesDrug Study Case AnalysisNine SaguiboNo ratings yet
- Study Guide for NLN RN Pharmacology ExamDocument64 pagesStudy Guide for NLN RN Pharmacology Exammaniz442No ratings yet
- Drug Study - Colon CancerDocument4 pagesDrug Study - Colon Cancerbea pegadNo ratings yet
- Tolvaptan-Drug StudyDocument1 pageTolvaptan-Drug Studykaycelyn jimenez100% (2)
- F-IMNCI Chart BookletDocument45 pagesF-IMNCI Chart BookletGunda SrinivasNo ratings yet
- Thera Hypertension Pregnant Group 1 PDFDocument3 pagesThera Hypertension Pregnant Group 1 PDFJanet Jane de RidderNo ratings yet
- ENT Vertigo FINAL v0.41Document1 pageENT Vertigo FINAL v0.41Farmasi BhamadaNo ratings yet
- ACLS ChartDocument1 pageACLS ChartJev DespiNo ratings yet
- Narce Sn-Ii, Nocete Sn-Ii NCM 109-n (RLE) BSN-2A Instructor: Mr. Julie Bless Parcon, RN, MAN Drug StudyDocument2 pagesNarce Sn-Ii, Nocete Sn-Ii NCM 109-n (RLE) BSN-2A Instructor: Mr. Julie Bless Parcon, RN, MAN Drug StudyAlmera Rose NarceNo ratings yet
- RanitidineDocument2 pagesRanitidineMagdayao Romamea100% (1)
- EMS Treatment Protocols Section 9000 PDFDocument37 pagesEMS Treatment Protocols Section 9000 PDFKevin PadilloNo ratings yet
- Adult BradycardiaDocument1 pageAdult BradycardiaTista ApriyanaNo ratings yet
- MedicationsDocument63 pagesMedicationssaraNo ratings yet
- Medical EmergencyDocument3 pagesMedical EmergencyIbrar HumayunNo ratings yet
- Surgical Appendectomy Nursing CareDocument3 pagesSurgical Appendectomy Nursing CareRoel John Atamosa CasilacNo ratings yet
- 7. OxytocinDocument1 page7. OxytocinyeshaellatapucayNo ratings yet
- ACLS - Guidelines From 2005USADocument62 pagesACLS - Guidelines From 2005USAsbontchevNo ratings yet
- Things To Look For During Morning RoundDocument3 pagesThings To Look For During Morning RoundTom YipNo ratings yet
- 014 Drug StudyDocument3 pages014 Drug StudyGrey KnighttNo ratings yet
- Davao Doctor Drug Study Program CriteriaDocument3 pagesDavao Doctor Drug Study Program Criteriakkd nyleNo ratings yet
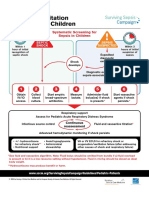
- Initial Resuscitation Algorithm For Children - Pdf.aspxDocument2 pagesInitial Resuscitation Algorithm For Children - Pdf.aspxasniatkoNo ratings yet
- Ketorolac, Pregabalin, Metoprolol nursing considerationsDocument4 pagesKetorolac, Pregabalin, Metoprolol nursing considerationsgayeng04No ratings yet
- Generic Name Indication Classification Pharmacokinetics Nursing ConsiderationDocument5 pagesGeneric Name Indication Classification Pharmacokinetics Nursing Considerationjoy rachel tabernillaNo ratings yet
- Drug StudyDocument3 pagesDrug Studyanne_ayala_1No ratings yet
- Drug StudyDocument11 pagesDrug StudyKeanu PeraltaNo ratings yet
- كيفيه التصرف في الحالات المختلفه في الاستقبالDocument91 pagesكيفيه التصرف في الحالات المختلفه في الاستقبالمحمد سعدون موسى عزيزNo ratings yet
- Aag Drug StudyDocument7 pagesAag Drug StudyAudrie Allyson GabalesNo ratings yet
- Enalapril, Metropolol, Aspirin, CiticolineDocument8 pagesEnalapril, Metropolol, Aspirin, CiticolineGabriel MatibagNo ratings yet
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- Early Prediction of Poststroke Rehabilitation Outcomes Using Wearable SensorsDocument33 pagesEarly Prediction of Poststroke Rehabilitation Outcomes Using Wearable SensorsGustavo CabanasNo ratings yet
- Biomechanical Properties of Fascial Tissues and Their RoleDocument3 pagesBiomechanical Properties of Fascial Tissues and Their RoleGustavo Cabanas100% (1)
- Cervical RadiculopathyDocument181 pagesCervical RadiculopathyE=MC2100% (2)
- Hedman 2018Document8 pagesHedman 2018Gustavo CabanasNo ratings yet
- Biology of Tendon Injury: Healing, Modeling and Remodeling: P. Sharma and N. MaffulliDocument10 pagesBiology of Tendon Injury: Healing, Modeling and Remodeling: P. Sharma and N. MaffulliBrianna RyanNo ratings yet
- Blood-Brain Barrier Dysfunction and Recovery Afte PDFDocument109 pagesBlood-Brain Barrier Dysfunction and Recovery Afte PDFGustavo CabanasNo ratings yet
- Corticospinal Excitability During Fatiguing Whole Body Exercise PDFDocument28 pagesCorticospinal Excitability During Fatiguing Whole Body Exercise PDFahokanoNo ratings yet
- Cervical Joint DysfunctionDocument5 pagesCervical Joint DysfunctionGustavo CabanasNo ratings yet
- Algorithmic Lumbar Decision MakingDocument10 pagesAlgorithmic Lumbar Decision MakingGustavo CabanasNo ratings yet
- Mechanisms of AxonDocument8 pagesMechanisms of AxonGustavo CabanasNo ratings yet
- Oligodendrocytes Biology and PathologyDocument17 pagesOligodendrocytes Biology and PathologyGustavo CabanasNo ratings yet
- Do Children Really Recover BetterDocument25 pagesDo Children Really Recover BetterGustavo CabanasNo ratings yet
- 9 Things To Know About ExerciseDocument4 pages9 Things To Know About ExerciseGustavo CabanasNo ratings yet
- SinapsisDocument4 pagesSinapsisGustavo CabanasNo ratings yet
- PDFDocument3 pagesPDFGustavo CabanasNo ratings yet
- Multiple Sclerosis OverviewDocument26 pagesMultiple Sclerosis OverviewGustavo CabanasNo ratings yet
- Anatomical Substrates of Oculomotor Control: Jean A Btittner-Ennever and Anja KE HorntDocument8 pagesAnatomical Substrates of Oculomotor Control: Jean A Btittner-Ennever and Anja KE HorntGustavo CabanasNo ratings yet
- 9 Things To Know About ExerciseDocument4 pages9 Things To Know About ExerciseGustavo CabanasNo ratings yet
- Locational Descriptions of Human Brodmann AreasDocument7 pagesLocational Descriptions of Human Brodmann AreasMark Anthony RaymundoNo ratings yet
- Somatosensory Processes Subserving Perception and ActionDocument51 pagesSomatosensory Processes Subserving Perception and ActionGustavo CabanasNo ratings yet
- 2 Types Functional Capacity EvaluationDocument6 pages2 Types Functional Capacity EvaluationGustavo CabanasNo ratings yet
- A Model For The Evolution of Decussation PDFDocument5 pagesA Model For The Evolution of Decussation PDFGustavo CabanasNo ratings yet
- Mechanisms of Action of Vagus Nerve StimulaDocument9 pagesMechanisms of Action of Vagus Nerve StimulaGustavo CabanasNo ratings yet
- Allodynia and Hyperalgesia in Neuropathic Pain PDFDocument12 pagesAllodynia and Hyperalgesia in Neuropathic Pain PDFGustavo CabanasNo ratings yet
- AFO OrtesisDocument59 pagesAFO OrtesisGustavo CabanasNo ratings yet
- Somatosensory Processes Subserving Perception and ActionDocument51 pagesSomatosensory Processes Subserving Perception and ActionGustavo CabanasNo ratings yet
- FasciaDocument53 pagesFasciaGustavo CabanasNo ratings yet
- Anodal TDCS Over M1Document9 pagesAnodal TDCS Over M1Gustavo CabanasNo ratings yet
- Cutaneous MelanomaDocument226 pagesCutaneous MelanomaGriskalia ChristineNo ratings yet
- Classification of FracturesDocument26 pagesClassification of FracturesHoney May Rollan VicenteNo ratings yet
- Tall StatureDocument24 pagesTall StaturedianmutiaNo ratings yet
- Psik Soal UtsDocument1 pagePsik Soal UtsNaurahSalsabil / 20No ratings yet
- Soal Final Nursing 2019-2020Document2 pagesSoal Final Nursing 2019-2020A.Tisna RamadhaniNo ratings yet
- 2018 Conference AbstractsDocument155 pages2018 Conference AbstractsBanin AbadiNo ratings yet
- تجميعات باثولوجيDocument3 pagesتجميعات باثولوجيTurky TurkyNo ratings yet
- Breast and Nipple Thrush - 280720Document6 pagesBreast and Nipple Thrush - 280720Robbie WilliamsNo ratings yet
- History, Diagnosis and Treatment Planning in Removable Partial DenturesDocument96 pagesHistory, Diagnosis and Treatment Planning in Removable Partial DenturesPriya BagalNo ratings yet
- Eeg, PSG, Sleep DisordersDocument48 pagesEeg, PSG, Sleep DisordersIoana MunteanuNo ratings yet
- Dr. Ayesha Latif's Guide to Airway ManagementDocument32 pagesDr. Ayesha Latif's Guide to Airway ManagementAyesha LatifNo ratings yet
- DR - Datten Bangun MSC - SPFK & DR - Tri Widyawati Msi, PHD Dept - Farmakologi & Therapeutik Fak - Kedokteran Usu MedanDocument50 pagesDR - Datten Bangun MSC - SPFK & DR - Tri Widyawati Msi, PHD Dept - Farmakologi & Therapeutik Fak - Kedokteran Usu MedanHabib Al KahfiNo ratings yet
- Probiotics vs Prebiotics: Differences, Advantages, TrendsDocument5 pagesProbiotics vs Prebiotics: Differences, Advantages, TrendsNaevisweloveuNo ratings yet
- Trigeminal Neuralgia GuideDocument15 pagesTrigeminal Neuralgia Guideandreas kevinNo ratings yet
- NP 5 Set BBBBBDocument31 pagesNP 5 Set BBBBBGo IdeasNo ratings yet
- Coliform BacteriaDocument4 pagesColiform BacteriaLalu Novan SatriaNo ratings yet
- Cap MRDocument4 pagesCap MRKit BarcelonaNo ratings yet
- Taking Medical HistoryDocument2 pagesTaking Medical HistoryDiana KulsumNo ratings yet
- Research Paper Brianna BartonDocument11 pagesResearch Paper Brianna Bartonapi-530899175No ratings yet
- Prevalence of Soil Transmitted Helminths infection in adults in North SulawesiDocument4 pagesPrevalence of Soil Transmitted Helminths infection in adults in North SulawesiSahrul hamidNo ratings yet
- History and P.E. of The Integumentary SystemDocument6 pagesHistory and P.E. of The Integumentary SystempazucenaNo ratings yet
- Atrial Fibrillation - Diagnosis and Treatment - AAFP PDFDocument8 pagesAtrial Fibrillation - Diagnosis and Treatment - AAFP PDFNaufal AmanullahNo ratings yet
- AntacidsDocument2 pagesAntacidsMa Corazon MelecioNo ratings yet
- Nerves Injury Post Neuroaxial AnesthesiaDocument11 pagesNerves Injury Post Neuroaxial AnesthesiaElisabeth SabajoNo ratings yet
- Thesis On HPV VaccineDocument8 pagesThesis On HPV Vaccinegjftqhnp100% (2)
- Prasugrel and RosuvastatinDocument7 pagesPrasugrel and RosuvastatinMohammad Shahbaz AlamNo ratings yet
- Strategi RS Dalam Pemenuhan Dan Pengaturan SDM CompressedDocument37 pagesStrategi RS Dalam Pemenuhan Dan Pengaturan SDM CompressedLilik SeptiyaNo ratings yet
- Comparative Efficacy of Non-Sedating Antihistamine Updosing in Patients With Chronic UrticariaDocument6 pagesComparative Efficacy of Non-Sedating Antihistamine Updosing in Patients With Chronic UrticariadregleavNo ratings yet