You might also like
- Schedule Cards The First Grade ParadeDocument48 pagesSchedule Cards The First Grade Paradevarna_gy100% (3)
- Pilot Trial of Hearingg Treatment For Reducing Cognitive Decline Results From The Aging and Cognitive Health Evaluation in Elders Pilot StudyDocument6 pagesPilot Trial of Hearingg Treatment For Reducing Cognitive Decline Results From The Aging and Cognitive Health Evaluation in Elders Pilot StudyDaniela Bustos PéndolaNo ratings yet
- The Effect of Tonguetie Division On Breasteeding and Speech ArticulationDocument12 pagesThe Effect of Tonguetie Division On Breasteeding and Speech ArticulationDaniela Bustos PéndolaNo ratings yet
- The Effects of Breastfeeding in Infants With PhenylketonuriaDocument6 pagesThe Effects of Breastfeeding in Infants With PhenylketonuriaDaniela Bustos PéndolaNo ratings yet
- Rinitis AlergicaDocument24 pagesRinitis AlergicaDaniela Bustos PéndolaNo ratings yet
- Pilot Trial of Hearingg Treatment For Reducing Cognitive Decline Results From The Aging and Cognitive Health Evaluation in Elders Pilot StudyDocument6 pagesPilot Trial of Hearingg Treatment For Reducing Cognitive Decline Results From The Aging and Cognitive Health Evaluation in Elders Pilot StudyDaniela Bustos PéndolaNo ratings yet
- Pilot Trial of Hearingg Treatment For Reducing Cognitive Decline Results From The Aging and Cognitive Health Evaluation in Elders Pilot StudyDocument6 pagesPilot Trial of Hearingg Treatment For Reducing Cognitive Decline Results From The Aging and Cognitive Health Evaluation in Elders Pilot StudyDaniela Bustos PéndolaNo ratings yet
- Delayed Breastfeeding Initiation Is Associated With Infant MorbidityDocument8 pagesDelayed Breastfeeding Initiation Is Associated With Infant MorbidityDaniela Bustos PéndolaNo ratings yet
- Audiologist N Patient Communication Profiles in Hearing RehabilitationDocument9 pagesAudiologist N Patient Communication Profiles in Hearing RehabilitationDaniela Bustos PéndolaNo ratings yet
- Association Between Brreastfeeding and Breathing Pattern in ChildrenDocument7 pagesAssociation Between Brreastfeeding and Breathing Pattern in ChildrenDaniela Bustos PéndolaNo ratings yet
- Breastfeeding and Language Outcomes A ReviweDocument12 pagesBreastfeeding and Language Outcomes A ReviweDaniela Bustos PéndolaNo ratings yet
- Chapter 3 Anatomical Organization of Cranial Nerves 2009 Manual Therapy For The Cranial NervesDocument4 pagesChapter 3 Anatomical Organization of Cranial Nerves 2009 Manual Therapy For The Cranial NervesDaniela Bustos PéndolaNo ratings yet
- Effects of A Musical Rhythmic Training On Children With Hearing LossDocument8 pagesEffects of A Musical Rhythmic Training On Children With Hearing LossDaniela Bustos PéndolaNo ratings yet
- Speech, Expressive Language in CP Iceland PDFDocument7 pagesSpeech, Expressive Language in CP Iceland PDFDaniela Bustos PéndolaNo ratings yet
- Intervencion en CF Paper 2008Document18 pagesIntervencion en CF Paper 2008Daniela Bustos PéndolaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- G6 - Report Project Highway Engineering - Section 2Document15 pagesG6 - Report Project Highway Engineering - Section 2alnz0% (1)
- Black Belt QuestionsDocument8 pagesBlack Belt QuestionsAbhirama B Sarepaka100% (1)
- MIA Case StudyDocument15 pagesMIA Case Studysujit89No ratings yet
- UK - Road To World Class ManufacturingDocument56 pagesUK - Road To World Class Manufacturinganji8388825No ratings yet
- AN0016 Applications of The Grad601 Magnetic GradiometerDocument2 pagesAN0016 Applications of The Grad601 Magnetic Gradiometerare7100% (1)
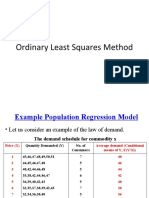
- OLS Regression Model ExplainedDocument72 pagesOLS Regression Model ExplainedHarishNo ratings yet
- The Mann Whitney U TestDocument4 pagesThe Mann Whitney U Testmnb0987No ratings yet
- Case Analysis QuestionsDocument7 pagesCase Analysis QuestionsAnkit DuttNo ratings yet
- Libqual+ From The Uk Perspective: Texas A&M UniversityDocument9 pagesLibqual+ From The Uk Perspective: Texas A&M UniversityBiNo ratings yet
- Guidelines For Environmental Risk Assessment and Management - 2011 - Green Leaves III - UKDocument9 pagesGuidelines For Environmental Risk Assessment and Management - 2011 - Green Leaves III - UKJosue RuaNo ratings yet
- Criminology, Law, and Justice (CLJ) : CoursesDocument2 pagesCriminology, Law, and Justice (CLJ) : CoursesJane Rose AlejadoNo ratings yet
- SPSS ProjectDocument12 pagesSPSS ProjectRishabh Sethi0% (1)
- Adolescent Mental HealthDocument50 pagesAdolescent Mental HealthmaiseducacaofisicaNo ratings yet
- APPLIED PSYCHOLOGY: FIELDS AND RESEARCHDocument5 pagesAPPLIED PSYCHOLOGY: FIELDS AND RESEARCHviji sathishNo ratings yet
- DMAIC Cycle Time ReductionDocument50 pagesDMAIC Cycle Time Reductionblitzkrig100% (1)
- Phương Pháp Nghiên C U Gi A KìDocument14 pagesPhương Pháp Nghiên C U Gi A KìVinh HoàngNo ratings yet
- Blooms Taxonomy Verb List PDFDocument2 pagesBlooms Taxonomy Verb List PDFSUGANTHINo ratings yet
- Customer Value Analysis PDFDocument7 pagesCustomer Value Analysis PDFpiyushsithaNo ratings yet
- Proposal of M.Ed. 4th SemesterDocument33 pagesProposal of M.Ed. 4th SemesterMan Bdr JoraNo ratings yet
- Savage Et Al. - 2013 - A New Model of Social Class Findings From The BBC S Great British Class Survey ExperimentDocument34 pagesSavage Et Al. - 2013 - A New Model of Social Class Findings From The BBC S Great British Class Survey ExperimentMaruclaNo ratings yet
- Relationship Between Parental Involvement and AP PerformanceDocument6 pagesRelationship Between Parental Involvement and AP PerformanceJudy Ann ChuaNo ratings yet
- Internship Report1Document31 pagesInternship Report1puneet guptaNo ratings yet
- Introduction To Business StatisticsDocument17 pagesIntroduction To Business StatisticsHammad MajidNo ratings yet
- Time Team - The Manor of The More, NorthwoodDocument58 pagesTime Team - The Manor of The More, NorthwoodWessex ArchaeologyNo ratings yet
- Job Descriptions ManualDocument36 pagesJob Descriptions ManualProf. Lakshman Madurasinghe100% (87)
- Robinson, H. S Et Al (2005), Business Performance Measurement Practices in Construction Engineering OrganisationsDocument28 pagesRobinson, H. S Et Al (2005), Business Performance Measurement Practices in Construction Engineering OrganisationsDavid SabaflyNo ratings yet
- Sensory Evaluation MethodsDocument10 pagesSensory Evaluation MethodsbatrisyiaNo ratings yet
- Hostel Life Impacts Personality and BehaviorDocument5 pagesHostel Life Impacts Personality and BehaviorHarsh Dwivedi100% (1)
- Updated Course Outline-BUS 201 - Section BDocument10 pagesUpdated Course Outline-BUS 201 - Section BNaseef Al Huq Bin RezaNo ratings yet
- Data-Informed Community-Focused Policing: in The Los Angeles Police DepartmentDocument27 pagesData-Informed Community-Focused Policing: in The Los Angeles Police DepartmentJake LanceNo ratings yet