You might also like
- Ezegboguand Abdulsalam 1Document8 pagesEzegboguand Abdulsalam 1TututWidyaNurAnggrainiNo ratings yet
- World Journal of Diabetes PDFDocument18 pagesWorld Journal of Diabetes PDFnikenauliaputriNo ratings yet
- Relationship between Family Support and Quality of Life in Diabetes PatientsDocument7 pagesRelationship between Family Support and Quality of Life in Diabetes PatientsTututWidyaNurAnggrainiNo ratings yet
- The Relationship Between Job Stress and PDFDocument9 pagesThe Relationship Between Job Stress and PDFTututWidyaNurAnggrainiNo ratings yet
- Diagnosis and Management of Panic Disorder in Adults: Locke AB., Kirst N.,2015. American Family Physician, 91 (9) :617-624Document14 pagesDiagnosis and Management of Panic Disorder in Adults: Locke AB., Kirst N.,2015. American Family Physician, 91 (9) :617-624TututWidyaNurAnggrainiNo ratings yet
- Prevalence and predictors of non-suicidal self-injury among children with autismDocument5 pagesPrevalence and predictors of non-suicidal self-injury among children with autismTututWidyaNurAnggrainiNo ratings yet
- Honey DropDocument5 pagesHoney DropdennisadityaNo ratings yet
- Ijbms 16 731Document12 pagesIjbms 16 731TututWidyaNurAnggrainiNo ratings yet
- Ijbms 16 731Document12 pagesIjbms 16 731TututWidyaNurAnggrainiNo ratings yet
- Non-Suicidal Self-Injury (NSSI) and Suicide: Criteria DifferentiationDocument7 pagesNon-Suicidal Self-Injury (NSSI) and Suicide: Criteria DifferentiationTututWidyaNurAnggrainiNo ratings yet
- Document PDFDocument6 pagesDocument PDFTututWidyaNurAnggrainiNo ratings yet
- Jurnal IkterusDocument3 pagesJurnal IkterusTututWidyaNurAnggrainiNo ratings yet
- Lio2 2 36Document7 pagesLio2 2 36MudrikahHaniyahNo ratings yet
- 161 321 1 SMDocument19 pages161 321 1 SMTututWidyaNurAnggrainiNo ratings yet
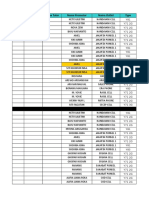
- Tanggal Area Nama Tutor Nama Promotor Nama Outlet TypeDocument32 pagesTanggal Area Nama Tutor Nama Promotor Nama Outlet TypeTututWidyaNurAnggrainiNo ratings yet
- 9 Autism Spectrum2Document29 pages9 Autism Spectrum2fauzanNo ratings yet
- SOAP BedahDocument2 pagesSOAP BedahTututWidyaNurAnggrainiNo ratings yet
- EpistaxisDocument23 pagesEpistaxisTututWidyaNurAnggrainiNo ratings yet
- SOAP BedahDocument2 pagesSOAP BedahTututWidyaNurAnggrainiNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Classification System For Oral Submucous FibrosisDocument6 pagesClassification System For Oral Submucous FibrosisMohamed FaizalNo ratings yet
- Defining Treatment Response, Remission, Relapse, and RecoveryDocument21 pagesDefining Treatment Response, Remission, Relapse, and Recovery주병욱No ratings yet
- Heart SoundDocument29 pagesHeart Sounddianpratiwirahim100% (1)
- HemorrhoidectomyDocument5 pagesHemorrhoidectomydrnareshkumar3281100% (1)
- Sample MCQs of VirologyDocument4 pagesSample MCQs of VirologyTemesgen Endalew100% (2)
- Pressure Ulcers Project - EditedDocument6 pagesPressure Ulcers Project - EditedZeera MohamadNo ratings yet
- Evolve Resources For Goulds Pathophysiology For The Health Professions 6th Edition Hubert Test BankDocument9 pagesEvolve Resources For Goulds Pathophysiology For The Health Professions 6th Edition Hubert Test Bankhungden8pne100% (26)
- Leukemias Nursing ManagementDocument20 pagesLeukemias Nursing ManagementAnusha Verghese100% (5)
- Renal FailureDocument4 pagesRenal FailureMunish DograNo ratings yet
- PIIS1053077021007862Document20 pagesPIIS1053077021007862RicardoNo ratings yet
- Understanding Radiation TherapyDocument24 pagesUnderstanding Radiation Therapyabhilashreddy45No ratings yet
- H&P Cheat SheetDocument3 pagesH&P Cheat SheetWilliam YangNo ratings yet
- Acne (Causes and Symptoms)Document4 pagesAcne (Causes and Symptoms)Siddharth ChoudheryNo ratings yet
- Gastroenterology - Lower GI Bleeding - SOAP Note - Maitreyi RamanDocument4 pagesGastroenterology - Lower GI Bleeding - SOAP Note - Maitreyi RamanFrancieudo Sampaio100% (1)
- COVID-19 Isolation Effects on Mental Health and EconomyDocument10 pagesCOVID-19 Isolation Effects on Mental Health and EconomyRimsHa ShAbbirNo ratings yet
- AmenorrheaDocument11 pagesAmenorrheaDr.med SurduckiNo ratings yet
- Lipo Contrast Cryo BrochureDocument5 pagesLipo Contrast Cryo BrochureSerenity ZhangNo ratings yet
- PDF Tablet Lepas LambatDocument13 pagesPDF Tablet Lepas Lambatannisya bubblesNo ratings yet
- FOP: Fibrodysplasia Ossificans ProgressivaDocument20 pagesFOP: Fibrodysplasia Ossificans ProgressivaAnnizaAgustinaNo ratings yet
- Dentigerous Cyst RadiolucencyDocument25 pagesDentigerous Cyst RadiolucencyDr. Deepanshi SutariaNo ratings yet
- Asking-Filling in Medical ReportDocument5 pagesAsking-Filling in Medical ReportMiss Hanay VinnyNo ratings yet
- Hypo Kale MiaDocument13 pagesHypo Kale MiaMuhammad IqbalNo ratings yet
- Abdominal Pain Case PresentationDocument52 pagesAbdominal Pain Case PresentationNico Avellana100% (1)
- Basic Objectives of Color and Spectral DopplerDocument5 pagesBasic Objectives of Color and Spectral DopplerAsaad Baloch100% (2)
- Three Cases of Chronic Suppurative Otitis Media (CSOM) Caused by Kerstersia Gyiorum and A Review of The LiteratureDocument6 pagesThree Cases of Chronic Suppurative Otitis Media (CSOM) Caused by Kerstersia Gyiorum and A Review of The LiteraturealdaNo ratings yet
- Burkitt's Lymphoma: A Guide to Diagnosis and TreatmentDocument51 pagesBurkitt's Lymphoma: A Guide to Diagnosis and TreatmentDee100% (2)
- Indications To Administer Special Tests: (1) Cochlear PathologyDocument11 pagesIndications To Administer Special Tests: (1) Cochlear PathologyASMAA NOORUDHEENNo ratings yet
- Ayurvedic Diabetes CureDocument13 pagesAyurvedic Diabetes CureYassine KrineNo ratings yet
- Is A Traditional Colonoscopy or A Virtual Colonoscopy BetterDocument1 pageIs A Traditional Colonoscopy or A Virtual Colonoscopy BetterPaul JensenNo ratings yet
- Measuring Dental DiseasesDocument19 pagesMeasuring Dental DiseasesmisdduaaNo ratings yet