You might also like
- Depression Conceptualization and Treatment: Dialogues from Psychodynamic and Cognitive Behavioral PerspectivesFrom EverandDepression Conceptualization and Treatment: Dialogues from Psychodynamic and Cognitive Behavioral PerspectivesChristos CharisNo ratings yet
- Hallucinations in ChildrenDocument9 pagesHallucinations in ChildrenEnda RafiqohNo ratings yet
- Theory Use in Counseling Practice: Current Trends: Int J Adv CounsellingDocument16 pagesTheory Use in Counseling Practice: Current Trends: Int J Adv CounsellingWastiti AdiningrumNo ratings yet
- Prodromal SchizophreniaDocument13 pagesProdromal SchizophreniadizhalfaNo ratings yet
- Critique of CBT 2007 Richard J. Longmore & Michael WorrellDocument15 pagesCritique of CBT 2007 Richard J. Longmore & Michael WorrellCarpenle100% (1)
- Clinical Psychological Science 2016 Beck 2167702616628523Document24 pagesClinical Psychological Science 2016 Beck 2167702616628523memo leyNo ratings yet
- Prolonged Exposure Therapy - Past, Present, and FutureDocument5 pagesProlonged Exposure Therapy - Past, Present, and FutureKelly GCNo ratings yet
- Schizoaffective Disorder FactsheetDocument6 pagesSchizoaffective Disorder FactsheetYusnida RahmawatiNo ratings yet
- Ipt-Ast Fact Sheet Interpersonal Therapy For AdolescentsDocument2 pagesIpt-Ast Fact Sheet Interpersonal Therapy For Adolescentsapi-507192289No ratings yet
- Manual Psicoger SparDocument430 pagesManual Psicoger Sparpereiraboan9140No ratings yet
- Clinical Treatment GuidelinesDocument147 pagesClinical Treatment GuidelinesAzeera RohimiNo ratings yet
- Psychoeducation for Schizophrenia Patients and FamiliesDocument9 pagesPsychoeducation for Schizophrenia Patients and FamiliesvinodksahuNo ratings yet
- Co-Occurring DisordersDocument91 pagesCo-Occurring DisordersEmilyNo ratings yet
- What S in A Case Formulation PDFDocument10 pagesWhat S in A Case Formulation PDFNicole Flores MuñozNo ratings yet
- Existential and Person Centered TherapyDocument21 pagesExistential and Person Centered Therapyapi-326209227No ratings yet
- Psychiatry Notes For PGDocument8 pagesPsychiatry Notes For PGskycall28100% (1)
- Mullen Polksys ArticleDocument6 pagesMullen Polksys Articleapi-249796934No ratings yet
- A Dynamic Group For The ElderlyDocument12 pagesA Dynamic Group For The ElderlyjuaromerNo ratings yet
- DSM IV CodesDocument16 pagesDSM IV CodesporzelNo ratings yet
- Disorders RushedDocument40 pagesDisorders Rushedapi-391411195No ratings yet
- Panss ScoreDocument8 pagesPanss ScoretriaclaresiaNo ratings yet
- Panic DisorderDocument323 pagesPanic DisorderTabitha MuscasNo ratings yet
- DSM 5 Intellectual Disability Fact SheetDocument2 pagesDSM 5 Intellectual Disability Fact SheetMelissa Ortega MaguiñaNo ratings yet
- MHA CognitiveBehaviouralTherapyDocument148 pagesMHA CognitiveBehaviouralTherapypuneeth87100% (1)
- Excoriation FaqDocument1 pageExcoriation FaqaladininsaneNo ratings yet
- Epstein Assertiveness Skills InventoryDocument11 pagesEpstein Assertiveness Skills InventoryMirjana StevanovicNo ratings yet
- Future Directions in Post-Traumatic Stress Disorder: Marilyn P. Safi R Helene S. Wallach Albert "Skip" Rizzo EditorsDocument428 pagesFuture Directions in Post-Traumatic Stress Disorder: Marilyn P. Safi R Helene S. Wallach Albert "Skip" Rizzo EditorsDaniela DiazNo ratings yet
- Psy460 Ch07 HandoutDocument6 pagesPsy460 Ch07 HandoutDev PrashadNo ratings yet
- Wells Brief Cognitive Therapy For Social Phobia - A Case SeriesDocument8 pagesWells Brief Cognitive Therapy For Social Phobia - A Case SeriesjuaromerNo ratings yet
- A Filled-In Example: Schema Therapy Case Conceptualization FormDocument10 pagesA Filled-In Example: Schema Therapy Case Conceptualization FormKarinaNo ratings yet
- 2015 - Post-Traumatic Stress Disorder (Review)Document22 pages2015 - Post-Traumatic Stress Disorder (Review)Andrés Felipe SarmientoNo ratings yet
- Andre F. Carvalho, Eduard Vieta - The Treatment of Bipolar Disorder - Integrative Clinical Strategies and Future Directions (2017, Oxford University Press) PDFDocument545 pagesAndre F. Carvalho, Eduard Vieta - The Treatment of Bipolar Disorder - Integrative Clinical Strategies and Future Directions (2017, Oxford University Press) PDFniles13100% (1)
- Treatment Resistant OcdDocument70 pagesTreatment Resistant Ocddrkadiyala2100% (1)
- (Jan Olav Johannessen, Brian Martindale, Johan CulDocument321 pages(Jan Olav Johannessen, Brian Martindale, Johan CulVigneshwaran Vikki100% (2)
- Linking Assessment and TreatmentDocument37 pagesLinking Assessment and Treatmentaimee2oo8No ratings yet
- Psychopharmacology: Borderline Personality DisorderDocument7 pagesPsychopharmacology: Borderline Personality DisorderAwais FaridiNo ratings yet
- The Self With OthersDocument61 pagesThe Self With OthersJohnny Ortega Sy Reyes IINo ratings yet
- A Cognitive Approach To Panic de David M. Clark 1986Document10 pagesA Cognitive Approach To Panic de David M. Clark 1986Jeaniret YañezNo ratings yet
- Assessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.ArchanaaDocument62 pagesAssessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.Archanaadrkadiyala2No ratings yet
- 2005, Vol.23, Issues 4, Psychocutaneous DiseaseDocument162 pages2005, Vol.23, Issues 4, Psychocutaneous DiseaseRizweta DestinNo ratings yet
- (Doi 10.12968 - Bjon.1995.4.15.876) A. Farrington - Models of Clinical Supervision PDFDocument3 pages(Doi 10.12968 - Bjon.1995.4.15.876) A. Farrington - Models of Clinical Supervision PDFHendri HariadiNo ratings yet
- Concise Guide To Anxiety Disorders PDFDocument273 pagesConcise Guide To Anxiety Disorders PDFshafijanNo ratings yet
- Depression in Adults 58302785221Document47 pagesDepression in Adults 58302785221andreNo ratings yet
- L18 Behavior Therapy TechniquesDocument19 pagesL18 Behavior Therapy Techniqueshitendra das50% (2)
- Patterson Cognitive Behavioral Systems ApproachDocument14 pagesPatterson Cognitive Behavioral Systems ApproachSusana FossaNo ratings yet
- Cognitive Therapy in The Treatment of Low Self-Esteem: References ReprintsDocument10 pagesCognitive Therapy in The Treatment of Low Self-Esteem: References ReprintsSulaksono Dwi AriNo ratings yet
- Rational Emotive Behaviour TherapyDocument16 pagesRational Emotive Behaviour TherapyCharrise RamkissoonNo ratings yet
- Group Therapy Approaches for AddictionDocument5 pagesGroup Therapy Approaches for AddictionSandra Jefferson100% (1)
- Christine Cordle - The Use of Operant Self-Control in Compulsive Hair-PullingDocument4 pagesChristine Cordle - The Use of Operant Self-Control in Compulsive Hair-PullingIrving Pérez MéndezNo ratings yet
- Bernard Gallagher Cap. 5 Sociology of Mental IllnessDocument16 pagesBernard Gallagher Cap. 5 Sociology of Mental IllnessLaura CristinaNo ratings yet
- Narrative Cognitive Behavior Therapy For PsychosisDocument12 pagesNarrative Cognitive Behavior Therapy For PsychosisGanellNo ratings yet
- Overview of DBTDocument12 pagesOverview of DBTHeronimas ArneNo ratings yet
- Cognitive Behavior Theraphy PDFDocument20 pagesCognitive Behavior Theraphy PDFAhkam BloonNo ratings yet
- Obsessive Compulsive Spectrum DisordersDocument62 pagesObsessive Compulsive Spectrum Disordersdrkadiyala2No ratings yet
- Personality Disorders PDFDocument35 pagesPersonality Disorders PDFABHINAVNo ratings yet
- Treatment of Psychological Disorders: Short Answer QuestionsDocument2 pagesTreatment of Psychological Disorders: Short Answer QuestionsAbhi Shah100% (1)
- CBT Case Formulation as Therapeutic ProcessFrom EverandCBT Case Formulation as Therapeutic ProcessGiovanni Maria RuggieroNo ratings yet
- States and Processes for Mental Health: Advancing Psychotherapy EffectivenessFrom EverandStates and Processes for Mental Health: Advancing Psychotherapy EffectivenessNo ratings yet
- Wiadrowski 2001Document4 pagesWiadrowski 2001Ioana AntonesiNo ratings yet
- PharmacovigilanceinClinicalDentistry SCDocument6 pagesPharmacovigilanceinClinicalDentistry SCIoana AntonesiNo ratings yet
- Antibiotice Oxford 2019 PDFDocument23 pagesAntibiotice Oxford 2019 PDFAny AsNo ratings yet
- GH 08 661Document8 pagesGH 08 661Ioana AntonesiNo ratings yet
- Asero 2001Document5 pagesAsero 2001Ioana AntonesiNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument17 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsIoana AntonesiNo ratings yet
- GutDocument7 pagesGutIoana AntonesiNo ratings yet
- Clostridium 2Document6 pagesClostridium 2Ioana AntonesiNo ratings yet
- Atypical Serological Profile in Hepatitis B Virus InfectionDocument18 pagesAtypical Serological Profile in Hepatitis B Virus InfectionMai TuyếtNo ratings yet
- Kong 2000Document16 pagesKong 2000Ioana AntonesiNo ratings yet
- Important Daas 1Document17 pagesImportant Daas 1Ioana AntonesiNo ratings yet
- Clostridium 1Document7 pagesClostridium 1Ioana AntonesiNo ratings yet
- Chloramphenicol Toxicity A Review PDFDocument5 pagesChloramphenicol Toxicity A Review PDFIoana AntonesiNo ratings yet
- Types of Biological Variables: Shreemathi S. Mayya, Ashma D Monteiro, Sachit GanapathyDocument4 pagesTypes of Biological Variables: Shreemathi S. Mayya, Ashma D Monteiro, Sachit GanapathyIoana AntonesiNo ratings yet
- 2018 Annual Report Eudravigilance European Parliament Council Commission Reporting Period 1 January enDocument36 pages2018 Annual Report Eudravigilance European Parliament Council Commission Reporting Period 1 January enIoana AntonesiNo ratings yet
- Cost-of-illness studies: Measuring healthcare costs fact vs fictionDocument2 pagesCost-of-illness studies: Measuring healthcare costs fact vs fictionIoana AntonesiNo ratings yet
- Magiorakis Paper PDFDocument14 pagesMagiorakis Paper PDFSambili TonnyNo ratings yet
- PharmacovigilanceinClinicalDentistry SCDocument6 pagesPharmacovigilanceinClinicalDentistry SCIoana AntonesiNo ratings yet
- In The: Antimicrobial Resistance: Lessons From RomaniaDocument11 pagesIn The: Antimicrobial Resistance: Lessons From RomaniaIoana AntonesiNo ratings yet
- PharmacovigilanceinClinicalDentistry SCDocument6 pagesPharmacovigilanceinClinicalDentistry SCIoana AntonesiNo ratings yet
- Harauchi 2017Document6 pagesHarauchi 2017Ioana AntonesiNo ratings yet
- Chloramphenicol Toxicity Revisited PDFDocument7 pagesChloramphenicol Toxicity Revisited PDFIoana AntonesiNo ratings yet
- H3) Geriatric: Effects of A Procaine Preparation (Gerovital in Hospitalized Patients: A Double-Blind StudyDocument5 pagesH3) Geriatric: Effects of A Procaine Preparation (Gerovital in Hospitalized Patients: A Double-Blind StudyIoana AntonesiNo ratings yet
- Metilxantine PDFDocument566 pagesMetilxantine PDFIoana AntonesiNo ratings yet
- NitrofurantoinDocument9 pagesNitrofurantoinIoana AntonesiNo ratings yet
- Factors Affecting The Pharmacokinetics o PDFDocument9 pagesFactors Affecting The Pharmacokinetics o PDFIoana AntonesiNo ratings yet
- Comparison of Clindamycin and ChloramphenicolDocument5 pagesComparison of Clindamycin and ChloramphenicolIoana AntonesiNo ratings yet
- Handbook of NutritionDocument280 pagesHandbook of Nutritionkad91% (22)
- Magiorakis Paper PDFDocument14 pagesMagiorakis Paper PDFSambili TonnyNo ratings yet
- Chloramphenicol-A Review of Its Use in Clinical Practice PDFDocument13 pagesChloramphenicol-A Review of Its Use in Clinical Practice PDFM Ishaq Khan AnjumNo ratings yet
- Activity On Learning StylesDocument11 pagesActivity On Learning StylesMary AthenaNo ratings yet
- GRADE 8 English Lessons on The Ramayana and Rubaiyat of Omar KhayamDocument3 pagesGRADE 8 English Lessons on The Ramayana and Rubaiyat of Omar KhayamErold Tarvina100% (1)
- Assessment in Learning 1Document15 pagesAssessment in Learning 1ana82% (17)
- Cmu F 1 Aca 005 (Nomination of Advisory Committee)Document2 pagesCmu F 1 Aca 005 (Nomination of Advisory Committee)RRNo ratings yet
- Hrm415 Midterm AssignmentDocument4 pagesHrm415 Midterm AssignmentJunaid AhnafNo ratings yet
- How A UPS Manager Cut TurnoverDocument4 pagesHow A UPS Manager Cut TurnoverShamaila Khan100% (1)
- DIG Presentation PDFDocument3 pagesDIG Presentation PDFDaniel Foster da SilvaNo ratings yet
- Lsl-Summerschool Presentation1Document8 pagesLsl-Summerschool Presentation1api-221804466No ratings yet
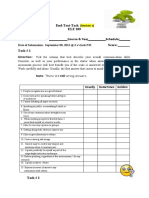
- End-Text-Task Communication Skills AssessmentDocument2 pagesEnd-Text-Task Communication Skills AssessmentRhayanstewart Gonzaga AdelantarNo ratings yet
- Living in Harmony with OthersDocument27 pagesLiving in Harmony with OthersFrancis Joseph Del Espiritu SantoNo ratings yet
- Teacher'S Portfolio: Jordan R. FernandezDocument7 pagesTeacher'S Portfolio: Jordan R. FernandezgdugangNo ratings yet
- 50 50 Strategies Strategies To Beat To Beat Anxiety Anxiety: Dr. Alice BoylesDocument5 pages50 50 Strategies Strategies To Beat To Beat Anxiety Anxiety: Dr. Alice BoylesAnonymous UNhoKel8m2No ratings yet
- The Importance of Self - and Shared Leadership in TDocument24 pagesThe Importance of Self - and Shared Leadership in TBrandon TanNo ratings yet
- Short Term Goals Vs Long Term Goals-2Document2 pagesShort Term Goals Vs Long Term Goals-2CIAN CARLO ANDRE TANNo ratings yet
- Sustaining ImprovementsDocument5 pagesSustaining Improvementsapi-4761895220% (1)
- A Beautiful MindDocument3 pagesA Beautiful Mindapi-31479794675% (4)
- Assignment 1 Inclusive Education EssayDocument9 pagesAssignment 1 Inclusive Education Essayapi-355889713No ratings yet
- Oliveira Et Al 2021Document19 pagesOliveira Et Al 2021Patricia Jara ReyesNo ratings yet
- 51 Ijmrp 3 (6) 263-65Document3 pages51 Ijmrp 3 (6) 263-65ahmed samirNo ratings yet
- Master of Education Models and Strategies of TeachingDocument37 pagesMaster of Education Models and Strategies of TeachingLeela Subramaniam Leela100% (1)
- Student Self Evaluation FormDocument2 pagesStudent Self Evaluation FormAwais RafiqNo ratings yet
- Picture DescriptionsDocument1 pagePicture DescriptionsVirginiaEspinosaNo ratings yet
- Authentic Assessment ToolsDocument19 pagesAuthentic Assessment Toolsmarygracejaspesiarot100% (1)
- Ca Teaching StandardsDocument1 pageCa Teaching Standardsapi-302779030100% (1)
- Task Based LearningDocument11 pagesTask Based LearningDaniel Martin50% (2)
- Leadership Theories HandoutDocument12 pagesLeadership Theories HandoutAnthony RiggsNo ratings yet
- Wellness - Anger ManagementDocument4 pagesWellness - Anger ManagementMind GateNo ratings yet
- Learning Styles ReflectionDocument2 pagesLearning Styles Reflectionapi-369996335No ratings yet
- Job Satisfaction Study of Employees at NHT Fashions LtdDocument14 pagesJob Satisfaction Study of Employees at NHT Fashions LtdSmart TvNo ratings yet
- Maslow Hierachy of Need Theory-231012 - 101119Document5 pagesMaslow Hierachy of Need Theory-231012 - 101119Rizz GynNo ratings yet