You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- 41 How To Cure DiseaseDocument60 pages41 How To Cure DiseaseEdie M Murgia0% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Chemotherapeutic Agents or Anti-MicrobialsDocument36 pagesChemotherapeutic Agents or Anti-MicrobialsPROF DR SHAHMURADNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Wound Care Basics: Types, Staging, Assessment & TreatmentDocument26 pagesWound Care Basics: Types, Staging, Assessment & TreatmentIntan Purnamasari100% (1)
- Surgical Site InfectionDocument14 pagesSurgical Site InfectionSri AsmawatiNo ratings yet
- Antimicrobial AgentsDocument3 pagesAntimicrobial AgentsErnie G. Bautista II, RN, MD100% (2)
- Preparation of Fortified Eye Drops: DR Sushmita G ShahDocument16 pagesPreparation of Fortified Eye Drops: DR Sushmita G Shahพานาที ลลันลาNo ratings yet
- Veterinary Drug Formulary GuideDocument245 pagesVeterinary Drug Formulary GuideAhmad Raza100% (4)
- Meropenem Drug StudyDocument2 pagesMeropenem Drug StudyPhoebe Guevarra100% (8)
- Infectious Disease GuideDocument33 pagesInfectious Disease GuideSilvia KesegNo ratings yet
- Stewardship Booklet Practical Guide To Antimicrobial Stewardship in HospitalsDocument23 pagesStewardship Booklet Practical Guide To Antimicrobial Stewardship in HospitalsZunisa Rizki100% (4)
- Mechanical Ventilation: Patient EducationDocument2 pagesMechanical Ventilation: Patient EducationAnis AidNo ratings yet
- From VAP To VAE: Establishing New Definitions For Ventilator-Associated Events in AdultsDocument22 pagesFrom VAP To VAE: Establishing New Definitions For Ventilator-Associated Events in AdultsJasleen KaurNo ratings yet
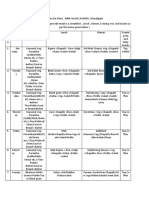
- Menu For MessDocument2 pagesMenu For MessJasleen KaurNo ratings yet
- Copd IntroDocument2 pagesCopd IntroSamuel JayNo ratings yet
- NowDocument1 pageNowJasleen KaurNo ratings yet
- ExercisesDocument4 pagesExercisesJasleen KaurNo ratings yet
- Ham A PDFDocument2 pagesHam A PDFHanum Maftukha100% (1)
- TABLE 11-1 - Compensatory Responses To Antihypertensive DrugsDocument1 pageTABLE 11-1 - Compensatory Responses To Antihypertensive DrugsJasleen KaurNo ratings yet
- Needs Assessment Questionnaire For CaregiversDocument4 pagesNeeds Assessment Questionnaire For CaregiversJasleen KaurNo ratings yet
- Total Knee Replacement Manual and Therapy/Rehab Protocol: Dr. Edward Kelly, MD, MBADocument12 pagesTotal Knee Replacement Manual and Therapy/Rehab Protocol: Dr. Edward Kelly, MD, MBAJasleen KaurNo ratings yet
- Blood Products and Their IndicationsDocument33 pagesBlood Products and Their IndicationsJasleen KaurNo ratings yet
- Role of Nurses in Triage and Disaster Preparedness: Workshop OnDocument2 pagesRole of Nurses in Triage and Disaster Preparedness: Workshop OnJasleen KaurNo ratings yet
- Table Common MedsDocument5 pagesTable Common Medsdanielc503No ratings yet
- Pulmonary Embolism: Amina Adel Al-QaysiDocument37 pagesPulmonary Embolism: Amina Adel Al-QaysiJasleen Kaur100% (2)
- Chest: Postgraduate Education CornerDocument8 pagesChest: Postgraduate Education CornerJasleen KaurNo ratings yet
- Measurement of CENTRAL VENOUS PRESSURE Via A TransducerDocument22 pagesMeasurement of CENTRAL VENOUS PRESSURE Via A TransducerJasleen KaurNo ratings yet
- 05 N044 42092Document18 pages05 N044 42092Jasleen KaurNo ratings yet
- Neocon 2017Document71 pagesNeocon 2017Jasleen KaurNo ratings yet
- 7ASTHMAPDocument10 pages7ASTHMAPErwin BawonoNo ratings yet
- Positive ETA culture and purulent secretions indicate probable VAPDocument1 pagePositive ETA culture and purulent secretions indicate probable VAPJasleen KaurNo ratings yet
- Dr. Clare Fenwick, 2010Document35 pagesDr. Clare Fenwick, 2010Jasleen KaurNo ratings yet
- CwsDocument25 pagesCwsJasleen KaurNo ratings yet
- 231Document9 pages231Jasleen KaurNo ratings yet
- The Gastrointestinal Tract and Ventilator-Associated PneumoniaDocument14 pagesThe Gastrointestinal Tract and Ventilator-Associated PneumoniaJasleen KaurNo ratings yet
- Pulmonary Embolism Is A Common and Potentially Lethal ConditionDocument13 pagesPulmonary Embolism Is A Common and Potentially Lethal ConditionJasleen KaurNo ratings yet
- YearbookDocument52 pagesYearbookJasleen KaurNo ratings yet
- Measuring Functional Progress after Hip ReplacementDocument7 pagesMeasuring Functional Progress after Hip ReplacementJasleen KaurNo ratings yet
- 7ASTHMAPDocument10 pages7ASTHMAPErwin BawonoNo ratings yet
- Ham A PDFDocument2 pagesHam A PDFHanum Maftukha100% (1)
- Augmentin in JDocument15 pagesAugmentin in JChutharat SucharitNo ratings yet
- Multiple Species: Section 2.1Document10 pagesMultiple Species: Section 2.1WormInchNo ratings yet
- DR Retno Budiarti, DR., M.Kes Microbiology Department FK UhtDocument45 pagesDR Retno Budiarti, DR., M.Kes Microbiology Department FK UhtalyaNo ratings yet
- Recommended Antibiotic Therapy in Severe Sepsis or Septic ShockDocument4 pagesRecommended Antibiotic Therapy in Severe Sepsis or Septic ShockBoy ReynaldiNo ratings yet
- NCLEX REVIEW AntibioticsDocument7 pagesNCLEX REVIEW Antibioticsneonstar100% (1)
- Antibacterial Activity of Aloe Vera Gel Against Multidrug Resistant Staphylococcus Aureus and Pseudomonas AeruginosaDocument7 pagesAntibacterial Activity of Aloe Vera Gel Against Multidrug Resistant Staphylococcus Aureus and Pseudomonas AeruginosaUMYU Journal of Microbiology Research (UJMR)100% (1)
- Careplan Week2Document2 pagesCareplan Week2api-302138606No ratings yet
- Phytoalexins PhytoanticipinsDocument3 pagesPhytoalexins PhytoanticipinsSébastien BellowNo ratings yet
- IDSA Guidelines for Managing Complicated Intra-abdominal InfectionsDocument32 pagesIDSA Guidelines for Managing Complicated Intra-abdominal InfectionsSylvain ColluraNo ratings yet
- Microbial Keratitis Royal College of OphthalmologistDocument2 pagesMicrobial Keratitis Royal College of OphthalmologistmahadianNo ratings yet
- Nama Prinsipal Kode Produk Nama Produk Unit Stok HnappnDocument4 pagesNama Prinsipal Kode Produk Nama Produk Unit Stok HnappnNoperitaNo ratings yet
- Opportunity, Challenge and Scope of Natural Products in Medicinal ChemistryDocument434 pagesOpportunity, Challenge and Scope of Natural Products in Medicinal ChemistryCamilla Karen Fernandes Carneiro100% (1)
- Antimicrobial Susceptibility Trends Among Gram-Negative Bacilli Causing Bloodstream Infections Results From The China Antimicrobial Resistance Surveillance Trial (CARST) Program, 2011-2020Document13 pagesAntimicrobial Susceptibility Trends Among Gram-Negative Bacilli Causing Bloodstream Infections Results From The China Antimicrobial Resistance Surveillance Trial (CARST) Program, 2011-2020Mrcom HvqyNo ratings yet
- Drug Information Bulletin 39 05Document4 pagesDrug Information Bulletin 39 05amritaryaaligarghNo ratings yet
- Mcqs 6Document19 pagesMcqs 6Muhammad JavedNo ratings yet
- 01.Guideline Idsa การรักษา Esbl, Cre, Mdr-psa (2021)Document44 pages01.Guideline Idsa การรักษา Esbl, Cre, Mdr-psa (2021)Nattawat TeerawattanapongNo ratings yet
- Panchagavya (Uses Benefits and Preparation)Document16 pagesPanchagavya (Uses Benefits and Preparation)Shreya VermaNo ratings yet
- MC Great Lakes SlidesDocument26 pagesMC Great Lakes Slidesapi-666654042No ratings yet
- Ous Microstrep Plus: Answers For LifeDocument2 pagesOus Microstrep Plus: Answers For LifeJimboreanu György PaulaNo ratings yet
- Cephalosporins: A Brief Overview of Their Chemistry, Mechanism of Action, and ClassificationDocument34 pagesCephalosporins: A Brief Overview of Their Chemistry, Mechanism of Action, and ClassificationTasnim sarairehNo ratings yet
- Antibiotics 1038832656Document20 pagesAntibiotics 1038832656Achilles Ok OkNo ratings yet