You might also like
- Advances in Awareness Monitoring TechnologiesDocument6 pagesAdvances in Awareness Monitoring TechnologiesEdwin SanchezNo ratings yet
- Remote and Longterm Selfmonitoring of Electroencephalographic and Noninvasive Measurable Variables at Home in Patients With Epilepsy EEGHOME Protocol For An Observational studyJMIR Research ProtocolsDocument12 pagesRemote and Longterm Selfmonitoring of Electroencephalographic and Noninvasive Measurable Variables at Home in Patients With Epilepsy EEGHOME Protocol For An Observational studyJMIR Research ProtocolsMiguel PalacioNo ratings yet
- Video and Ambulatory EEG Monitoring in The Diagnosis of Seizures and Epilepsy - UpToDateDocument20 pagesVideo and Ambulatory EEG Monitoring in The Diagnosis of Seizures and Epilepsy - UpToDateAndres Rojas JerezNo ratings yet
- Wagner2022 Article EfficacyAndSafetyOfIntravenousDocument13 pagesWagner2022 Article EfficacyAndSafetyOfIntravenoustito reddyNo ratings yet
- Superiority of Continuous Over Intermittent Intraoperative Nerve Monitoring in Preventing Vocal Cord PalsyDocument9 pagesSuperiority of Continuous Over Intermittent Intraoperative Nerve Monitoring in Preventing Vocal Cord PalsyazharbattooNo ratings yet
- Current Opinion Neurology ED 2019 Zwergal PDFDocument10 pagesCurrent Opinion Neurology ED 2019 Zwergal PDFveronikiNo ratings yet
- Bmjopen 2017 019073Document6 pagesBmjopen 2017 019073Makhda Nurfatmala LubisNo ratings yet
- Safety Ra PediatricsDocument6 pagesSafety Ra PediatricsDellNo ratings yet
- Vagus Nerve Stimulation in The Treatment of Drug Resistant Epilepsy in 29 Children 2016 European Journal of Paediatric NeurologyDocument6 pagesVagus Nerve Stimulation in The Treatment of Drug Resistant Epilepsy in 29 Children 2016 European Journal of Paediatric NeurologyZeptalanNo ratings yet
- Vertigo MeniereDocument5 pagesVertigo MeniereHamba AllahNo ratings yet
- IncidenceDocument11 pagesIncidenceNenad ProdanovicNo ratings yet
- Critical Care Medicine: Background: Methods: ResultsDocument9 pagesCritical Care Medicine: Background: Methods: ResultsMedicina InternaNo ratings yet
- Clinical Management of Seizures in Newborns: Diagnosis and TreatmentDocument10 pagesClinical Management of Seizures in Newborns: Diagnosis and TreatmentfitriNo ratings yet
- Santoso 2020Document10 pagesSantoso 2020Aldo VictoriaNo ratings yet
- 1 s2.0 S0165587617302975 Main PDFDocument4 pages1 s2.0 S0165587617302975 Main PDFAchmad YunusNo ratings yet
- Garin 2015Document9 pagesGarin 2015Thya84No ratings yet
- 1 s2.0 S1059131121001692 MainDocument9 pages1 s2.0 S1059131121001692 MainsoylahijadeunvampiroNo ratings yet
- 2023 - Pitfalls in Scalp EEG - Current Obstacles and Future Directions - SandorDocument21 pages2023 - Pitfalls in Scalp EEG - Current Obstacles and Future Directions - SandorJose Carlos Licea BlancoNo ratings yet
- Neonatal Seizures: Incidence, Etiologies, Clinical Features and EEG Findings in The Neonatal Intensive Care UnitDocument5 pagesNeonatal Seizures: Incidence, Etiologies, Clinical Features and EEG Findings in The Neonatal Intensive Care UnitDoraemon BiruNo ratings yet
- Neurosci 05 00004Document12 pagesNeurosci 05 00004G GggNo ratings yet
- NiceDocument7 pagesNiceRisky Ilona SaputraNo ratings yet
- Opsoclonus-Myoclonus in Children Associated or Not With NeuroblastomaDocument10 pagesOpsoclonus-Myoclonus in Children Associated or Not With Neuroblastomapengchuan72No ratings yet
- 1.diagnostic Long Term Video EEGDocument4 pages1.diagnostic Long Term Video EEGannaNo ratings yet
- Extubation Success Prediction in A Multicentric Cohort of Patients With Severe Brain InjuryDocument9 pagesExtubation Success Prediction in A Multicentric Cohort of Patients With Severe Brain InjuryEdison LucioNo ratings yet
- Expert Systems With Applications: Tarig Faisal, Mohd Nasir Taib, Fatimah IbrahimDocument13 pagesExpert Systems With Applications: Tarig Faisal, Mohd Nasir Taib, Fatimah IbrahimDwi Rahma YunikaNo ratings yet
- Minimizing Artifact Induced False Alarms For Seizure Detection in Wearable EEG Devices With Gradient Boosted Tree ClassifiersDocument16 pagesMinimizing Artifact Induced False Alarms For Seizure Detection in Wearable EEG Devices With Gradient Boosted Tree ClassifiersG GggNo ratings yet
- Hypothermia For Neuroprotection in Convulsive Status EpilepticusDocument11 pagesHypothermia For Neuroprotection in Convulsive Status EpilepticusismaangrianiNo ratings yet
- AygunDocument5 pagesAygunotheasNo ratings yet
- Cochlear Implantation Under Local Anesthesia and Conscious Sedation: An Italian ExperienceDocument6 pagesCochlear Implantation Under Local Anesthesia and Conscious Sedation: An Italian ExperiencePritam PanigrahiNo ratings yet
- Lucas 2014Document8 pagesLucas 2014Prima YosiNo ratings yet
- Predictive Factors For Recovery in Idiopathic Sudden Sensory Neural Hearing LossDocument8 pagesPredictive Factors For Recovery in Idiopathic Sudden Sensory Neural Hearing LossMiss AmyNo ratings yet
- Extubation Readiness in Critically Ill Stroke PatientsDocument8 pagesExtubation Readiness in Critically Ill Stroke PatientsMedicina InternaNo ratings yet
- Predictive Factors For Postoperative Outcome in Temporal Lobe Epilepsy According To Two Different ClassificationsDocument12 pagesPredictive Factors For Postoperative Outcome in Temporal Lobe Epilepsy According To Two Different ClassificationsPrabaningrum DwidjoasmoroNo ratings yet
- P300 in Patients With Epilepsy - The DifDocument241 pagesP300 in Patients With Epilepsy - The DifasasakopNo ratings yet
- Seizure: Kristina Malmgren, Anna EdelvikDocument8 pagesSeizure: Kristina Malmgren, Anna EdelvikRidho ArendoNo ratings yet
- Neuro-Ophthalmological Biomarkers of Visual Outcome in Newly Diagnosed Idiopathic Intracranial HypertensionDocument8 pagesNeuro-Ophthalmological Biomarkers of Visual Outcome in Newly Diagnosed Idiopathic Intracranial HypertensionMira TamilaNo ratings yet
- JPM 13 01411 v2Document15 pagesJPM 13 01411 v2Luluil MunirohNo ratings yet
- 1 s2.0 S1059131117306799 MainDocument7 pages1 s2.0 S1059131117306799 MainBruno NdoumouNo ratings yet
- Correlation of Visual Field Defects and Optical Coherence Tomography Finding in Migraine PatientsDocument5 pagesCorrelation of Visual Field Defects and Optical Coherence Tomography Finding in Migraine Patientsmara 11No ratings yet
- Hongliang Mao Short and Long Term Response of VagusDocument16 pagesHongliang Mao Short and Long Term Response of VagusArbey Aponte PuertoNo ratings yet
- 1 s2.0 S2255482312702126 MainDocument9 pages1 s2.0 S2255482312702126 MainsarinovitapratiwiNo ratings yet
- ScreeningDocument7 pagesScreeningRozalinaNo ratings yet
- 1 s2.0 S1059131120303162 MainDocument9 pages1 s2.0 S1059131120303162 MainInes Arias PazNo ratings yet
- Imedpub Journals 2018 2018Document6 pagesImedpub Journals 2018 2018jemyNo ratings yet
- Behdad Et Al-2009-EpilepsiaDocument12 pagesBehdad Et Al-2009-EpilepsiaNathaly LapoNo ratings yet
- Current Status of Continuous Electroencephalographic Monitoring in Critically Ill ChildrenDocument7 pagesCurrent Status of Continuous Electroencephalographic Monitoring in Critically Ill ChildrenMauricio RiveraNo ratings yet
- 2020karoly SeizurediaryforecastingDocument11 pages2020karoly SeizurediaryforecastingLevin KuhlmannNo ratings yet
- The Silent Gap Between Epilepsy Surgery Evaluations and Clinical Practice GuidelinesDocument2 pagesThe Silent Gap Between Epilepsy Surgery Evaluations and Clinical Practice GuidelinesAmelia PratiwiNo ratings yet
- Epilepsy Duration and Seizure Outcome in Epilepsy Surgery: A Systematic Review and Meta-AnalysisDocument9 pagesEpilepsy Duration and Seizure Outcome in Epilepsy Surgery: A Systematic Review and Meta-Analysisbaba ababNo ratings yet
- 2017 Results of Endoscopically-Assisted Cubital Tunnel Release Without Using Any Specific InstrumentDocument4 pages2017 Results of Endoscopically-Assisted Cubital Tunnel Release Without Using Any Specific InstrumentDimitris RodriguezNo ratings yet
- Applied Sciences: Respiration Monitoring For Premature Neonates in NicuDocument11 pagesApplied Sciences: Respiration Monitoring For Premature Neonates in NicuNicole LantinNo ratings yet
- Seizure: Caryn Jory, Rohit Shankar, Deborah Coker, Brendan Mclean, Jane Hanna, Craig NewmanDocument12 pagesSeizure: Caryn Jory, Rohit Shankar, Deborah Coker, Brendan Mclean, Jane Hanna, Craig NewmanNEHA BHATINo ratings yet
- Misljenja Medicinskih Sestra I Tehnicara o Izvjescivanju o Nezeljenim Dogadajima Tijekom Procesa Sestrinske SkrbiDocument15 pagesMisljenja Medicinskih Sestra I Tehnicara o Izvjescivanju o Nezeljenim Dogadajima Tijekom Procesa Sestrinske SkrbiStanislava RokvicNo ratings yet
- MMF in TEDDocument12 pagesMMF in TEDAfnindyas AtikaNo ratings yet
- Clinical Study: Outcome and Prognostic Factors For Traumatic Endophthalmitis Over A 5-Year PeriodDocument8 pagesClinical Study: Outcome and Prognostic Factors For Traumatic Endophthalmitis Over A 5-Year PeriodannisaNo ratings yet
- Echography and Doppler of the BrainFrom EverandEchography and Doppler of the BrainChiara RobbaNo ratings yet
- 694-701 Yoeruek LoDocument8 pages694-701 Yoeruek LoMeirinda HidayantiNo ratings yet
- Vertigo Associated With Cochlear Implant Surgery: Correlation With Vertigo Diagnostic Result, Electrode Carrier, and Insertion AngleDocument18 pagesVertigo Associated With Cochlear Implant Surgery: Correlation With Vertigo Diagnostic Result, Electrode Carrier, and Insertion AngleSMA N 1 TOROHNo ratings yet
- 07 October 2021 Status Epilepticus Short Journal Article Stetefeld2021 - Article - IsofluraneInSuper-RefractoryStDocument9 pages07 October 2021 Status Epilepticus Short Journal Article Stetefeld2021 - Article - IsofluraneInSuper-RefractoryStMarkhum GoundenNo ratings yet
- Journal 3Document6 pagesJournal 3riskab123No ratings yet
- Miller DiekerDocument8 pagesMiller DiekerJucsy JuxyNo ratings yet
- Benzo Conversion TableDocument1 pageBenzo Conversion TableJucsy JuxyNo ratings yet
- Firmicutes Bacteroidetes Proteobacteria Actinobacteria Fusobacteria TM7Document1 pageFirmicutes Bacteroidetes Proteobacteria Actinobacteria Fusobacteria TM7Jucsy JuxyNo ratings yet
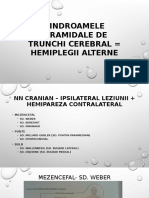
- Sindroamele Piramidale de Trunchi Cerebral Hemiplegii AlterneDocument9 pagesSindroamele Piramidale de Trunchi Cerebral Hemiplegii AlterneJucsy JuxyNo ratings yet
- Normal EEG Patterns in Infants A Children - Textbook.finalDocument11 pagesNormal EEG Patterns in Infants A Children - Textbook.finalJucsy JuxyNo ratings yet
- Viral EncephalitisDocument29 pagesViral Encephalitisruntika100% (1)
- MCQ 2019 Part 1 UseDocument94 pagesMCQ 2019 Part 1 UseWanny WattakavanichNo ratings yet
- Moonstruck? The Effect of The Lunar Cycle On SeizuresDocument2 pagesMoonstruck? The Effect of The Lunar Cycle On SeizuresArthur GomesNo ratings yet
- AustAlctreatguidelines 2009 PDFDocument255 pagesAustAlctreatguidelines 2009 PDFFrizam DwindamuldanNo ratings yet
- Seizure-Action Plan Epilepsy FoundationDocument1 pageSeizure-Action Plan Epilepsy FoundationRoxanne ReyNo ratings yet
- CHAPTER 19: Drugs Used For Seizure DisordersDocument19 pagesCHAPTER 19: Drugs Used For Seizure DisordersAziil LiizaNo ratings yet
- Pediatric Nursing Common ProblemsDocument33 pagesPediatric Nursing Common ProblemsMaricel Agcaoili GallatoNo ratings yet
- Epilepsy NotesDocument6 pagesEpilepsy NotesPrarthana Thiagarajan100% (1)
- IAF Medical Standards For PILOTSDocument43 pagesIAF Medical Standards For PILOTSBIJAY KUMAR ROUTNo ratings yet
- Rescue Treatment SeizuresDocument3 pagesRescue Treatment Seizureseko aNo ratings yet
- Febrile Seizures: Janith ChandrakumaraDocument14 pagesFebrile Seizures: Janith ChandrakumaraJanith ChandrakumaraNo ratings yet
- MCQ Neuro SampleDocument12 pagesMCQ Neuro SampleMutiara AdystiNo ratings yet
- Art and PsychoanalysisDocument434 pagesArt and PsychoanalysisdomingezNo ratings yet
- MSF Clinical Guidelines PDFDocument356 pagesMSF Clinical Guidelines PDFKirthinath BallalNo ratings yet
- Is Epilepsy Caused by Shaitan?Document3 pagesIs Epilepsy Caused by Shaitan?drsayeeduddinNo ratings yet
- Soal UjianDocument5 pagesSoal UjianApt RiskaNo ratings yet
- F1 - Manage ManualDocument32 pagesF1 - Manage ManualHasri LimbongNo ratings yet
- Battlefield 1942 - ManualDocument36 pagesBattlefield 1942 - ManualM_MolliNo ratings yet
- Manual ShipSimExtremes ENGDocument43 pagesManual ShipSimExtremes ENGAnonymous 1l8njobNo ratings yet
- Seizure Induced by Traumatic Brain Injury Case FileDocument7 pagesSeizure Induced by Traumatic Brain Injury Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Epilepsy & Behavior: Rachel Galioto, Andrew S. Blum, Geoffrey TremontDocument5 pagesEpilepsy & Behavior: Rachel Galioto, Andrew S. Blum, Geoffrey Tremontnaina sethNo ratings yet
- Complications of Brain Tumors and Their TreatmentDocument18 pagesComplications of Brain Tumors and Their TreatmentBenedictus Yudha BaskaraNo ratings yet
- The New Definition and Classification of Seizures and EpilepsyDocument16 pagesThe New Definition and Classification of Seizures and EpilepsynadiafyNo ratings yet
- Module 9Document12 pagesModule 9Augene ToribioNo ratings yet
- RCSI Course Book Chapters 22-27 Week 4Document75 pagesRCSI Course Book Chapters 22-27 Week 4BoyNo ratings yet
- Ramilo-Act 123Document4 pagesRamilo-Act 123Jayselle ArvieNo ratings yet
- Status EpilepticusDocument6 pagesStatus Epilepticussandykumala100% (1)
- Health and Safety For Preschool Children Lesson PlanDocument5 pagesHealth and Safety For Preschool Children Lesson PlanNika BuzonNo ratings yet
- Algorithm Febrile SeizuresDocument32 pagesAlgorithm Febrile SeizuresSi Puput100% (1)
- Mafia Ii 360 Download Manual EngDocument21 pagesMafia Ii 360 Download Manual EngJuan Camilo Payan GuerreroNo ratings yet