You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Cold War Lesson PlanDocument7 pagesCold War Lesson Planapi-311332271No ratings yet
- Document D - Atlanta Constitution-1Document2 pagesDocument D - Atlanta Constitution-1Rafael DevonishNo ratings yet
- Rights of Sewage Workers InterviewDocument8 pagesRights of Sewage Workers Interviewapi-541981758No ratings yet
- Latest Circular For Payment of Interest Free Festival Advance To StaffDocument1 pageLatest Circular For Payment of Interest Free Festival Advance To Staffhimadri_bhattacharjeNo ratings yet
- Social InequalityDocument2 pagesSocial InequalityElyza Marie CortezaNo ratings yet
- Case Analysis Samira Kohli vs. Prabha ManchandaDocument5 pagesCase Analysis Samira Kohli vs. Prabha ManchandaAshish JhaNo ratings yet
- Soce FormDocument22 pagesSoce Formjackbinayug8No ratings yet
- PALMARDocument7 pagesPALMARGrayshel Lampacan AoasNo ratings yet
- Developments in Business Simulation & Experiential Exercises, Volume 22, 1995Document4 pagesDevelopments in Business Simulation & Experiential Exercises, Volume 22, 1995AHMAD ALINo ratings yet
- Iv. The State: 1. National TerritoryDocument6 pagesIv. The State: 1. National TerritoryManuelMarasiganMismanosNo ratings yet
- Display PDF - PHPDocument21 pagesDisplay PDF - PHPanshulpatel0608No ratings yet
- Saklar NeroDocument9 pagesSaklar NeroIsmi Ambar SariNo ratings yet
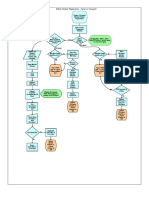
- Mobile Number Reg FlowchartDocument1 pageMobile Number Reg FlowchartKarthikayani PalaniNo ratings yet
- Credit Transactions (Mutuum)Document38 pagesCredit Transactions (Mutuum)Maestro LazaroNo ratings yet
- Congratulations On The Bonus Accrued!: Gajbhiye AmitkumarDocument2 pagesCongratulations On The Bonus Accrued!: Gajbhiye Amitkumaramit gajbhiyeNo ratings yet
- Moderator'S ScriptDocument3 pagesModerator'S ScriptElisha XDNo ratings yet
- Types of MigrationDocument5 pagesTypes of MigrationAngel ResusNo ratings yet
- Pastp PAPERSDocument3 pagesPastp PAPERSABDULLAH SAGHIRNo ratings yet
- Thoery of IR June Exam NotesDocument36 pagesThoery of IR June Exam NotesRalitsa HristovaNo ratings yet
- Oposa Law Office For Petitioners. The Solicitor General For RespondentsDocument14 pagesOposa Law Office For Petitioners. The Solicitor General For RespondentsJunior DaveNo ratings yet
- Print Application Form: Uttar PradeshDocument5 pagesPrint Application Form: Uttar PradeshManojNo ratings yet
- History of Colonialism and StruggleDocument11 pagesHistory of Colonialism and StruggleDL MolintasNo ratings yet
- G.R. No. 140756 - PEOPLE OF THE PHILIPPINES vs. JUAN GONZALES ESCOTE, ET ALDocument20 pagesG.R. No. 140756 - PEOPLE OF THE PHILIPPINES vs. JUAN GONZALES ESCOTE, ET ALLucy HeartfiliaNo ratings yet
- Lorenz 2022 Soro SokeDocument170 pagesLorenz 2022 Soro SokeThadonychusNo ratings yet
- Quinagoran v. CADocument4 pagesQuinagoran v. CAAce MarjorieNo ratings yet
- 199 Wajeeha 2k18 LLBDocument6 pages199 Wajeeha 2k18 LLBWajeeha LakhoNo ratings yet
- CCTV Systems: Merseyside Police - SeftonDocument10 pagesCCTV Systems: Merseyside Police - SeftonPERVEZ AHMAD KHANNo ratings yet
- How To Conduct A Workplace Investigation On Employee TheftDocument3 pagesHow To Conduct A Workplace Investigation On Employee TheftRommel SalalimaNo ratings yet
- RamachandraDocument2 pagesRamachandraVivek SettipalliNo ratings yet