You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- IV Induction Agents: Propofol, Ketamine, Etomidate, ThiopentoneDocument2 pagesIV Induction Agents: Propofol, Ketamine, Etomidate, ThiopentoneNdalilashiwa Penehafo Ndakondja-VictorNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- MED - Post Review ExamDocument8 pagesMED - Post Review ExamFrederick BallesterosNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Jurnal Pendukung 2Document13 pagesJurnal Pendukung 2Eko PrasNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Early Enteral NutritionDocument55 pagesEarly Enteral NutritionAdya ArradikhaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Lecture 4 Medical Terminology PDFDocument38 pagesLecture 4 Medical Terminology PDFAhmed KhaledNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Introduction To AnesthesiologyDocument68 pagesIntroduction To AnesthesiologyOzza AlhudaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- CRAFFTDocument24 pagesCRAFFTRani HusainNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Oral Cancer BDADocument36 pagesOral Cancer BDAJesús De Santos AlbaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Meningitis Beyond Neonatal AgeDocument57 pagesMeningitis Beyond Neonatal AgeTilahun Kegne100% (2)
- Antimicrobial ChemotherapyDocument160 pagesAntimicrobial Chemotherapyokumu atanas0% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Neuro 101: Nursing Neuro Assessment GuideDocument29 pagesNeuro 101: Nursing Neuro Assessment GuideDarvin MathewNo ratings yet
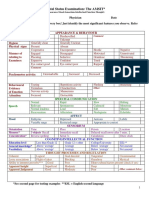
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledDocument2 pagesMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Ladewig 8e TIF Ch01 PDFDocument13 pagesLadewig 8e TIF Ch01 PDFjames smithNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Postpartum Complications: Donald G. Camatura, RNDocument96 pagesPostpartum Complications: Donald G. Camatura, RNDonald Garcesa Camatura100% (4)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Distalization of Maxillary Molars Using A Lever Arm and Mini-ImplantDocument10 pagesDistalization of Maxillary Molars Using A Lever Arm and Mini-ImplantYury Tenorio CahuanaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- ComplianceDocument13 pagesCompliancextremist2001No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Lab Technician or Clerical or BankingDocument2 pagesLab Technician or Clerical or Bankingapi-76931734No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Bumrungrad HospitalDocument3 pagesBumrungrad HospitalAhmadnur kholilNo ratings yet
- AplDocument37 pagesApladitiya tegarNo ratings yet
- Burnout Syndrome - in NursingDocument5 pagesBurnout Syndrome - in NursingIOSRjournalNo ratings yet
- ORTHOPAEDICS TRAUMADocument33 pagesORTHOPAEDICS TRAUMARhomizal MazaliNo ratings yet
- Tracheo-Oesophageal FistulaDocument19 pagesTracheo-Oesophageal Fistularajan kumar100% (3)
- Newborn Care PresentationDocument35 pagesNewborn Care PresentationChristian PallaviNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- RN Viray ResumefinalDocument1 pageRN Viray Resumefinalapi-661315652No ratings yet
- Gleason ScoreDocument7 pagesGleason ScoreClaudia KNo ratings yet
- Child With HematuriaDocument42 pagesChild With HematuriaalaaNo ratings yet
- Evaluación Habilidades Motoras Orales en NiñosDocument8 pagesEvaluación Habilidades Motoras Orales en NiñosSebastián Andrés ContrerasNo ratings yet
- Er LFD 11Document1 pageEr LFD 11EldwinCauilanNo ratings yet
- PericarditisDocument11 pagesPericarditisrbarcellonaNo ratings yet
- CLOZE TEST Discovery Could Ease Blood ShortageDocument2 pagesCLOZE TEST Discovery Could Ease Blood ShortageKarsan Ayaz MaierNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)