You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- India Today 29 June 2020 PDFDocument76 pagesIndia Today 29 June 2020 PDFJim Jose AntonyNo ratings yet
- 6min English Kids at Home PDFDocument5 pages6min English Kids at Home PDFJim Jose AntonyNo ratings yet
- 6min English Electricity PDFDocument5 pages6min English Electricity PDFJim Jose AntonyNo ratings yet
- Dr. Elham Bukhari: Aediatri Nfectious IseaseDocument56 pagesDr. Elham Bukhari: Aediatri Nfectious IseaseJim Jose AntonyNo ratings yet
- Immunization in Children: Fahad Al ZamilDocument44 pagesImmunization in Children: Fahad Al ZamilJim Jose AntonyNo ratings yet
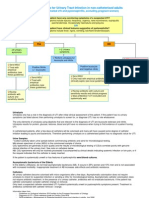
- Urinary Tract Infection in Children: Dr. Alia Al-Ibrahim Consultant Pediatric Nephrology Clinical Assistant ProfessorDocument11 pagesUrinary Tract Infection in Children: Dr. Alia Al-Ibrahim Consultant Pediatric Nephrology Clinical Assistant ProfessorJim Jose AntonyNo ratings yet
- Common Cutaneous Infections and InfestationsDocument28 pagesCommon Cutaneous Infections and InfestationsJim Jose AntonyNo ratings yet
- Acute Visual LossDocument10 pagesAcute Visual LossJim Jose AntonyNo ratings yet
- Cardiology Disease List PDFDocument139 pagesCardiology Disease List PDFJim Jose AntonyNo ratings yet
- Ortho Team FinalDocument221 pagesOrtho Team FinalJim Jose AntonyNo ratings yet
- Refractive ErrorsDocument7 pagesRefractive ErrorsJim Jose AntonyNo ratings yet
- Ocular EmergenciesDocument4 pagesOcular EmergenciesJim Jose AntonyNo ratings yet
- Strabismus, Amblyopia Management and LeukocoriaDocument19 pagesStrabismus, Amblyopia Management and LeukocoriaJim Jose AntonyNo ratings yet
- Optha: NeuroDocument13 pagesOptha: NeuroJim Jose AntonyNo ratings yet
- Chronic Visual LossDocument7 pagesChronic Visual LossJim Jose AntonyNo ratings yet
- COPD and BronchiectasisDocument20 pagesCOPD and BronchiectasisJim Jose AntonyNo ratings yet
- Pleural EffusionDocument10 pagesPleural EffusionJim Jose Antony100% (1)
- GoutDocument1 pageGoutJim Jose AntonyNo ratings yet
- Investigations of Lung DiseasesDocument14 pagesInvestigations of Lung DiseasesJim Jose AntonyNo ratings yet
- Orthopedic History Taking: DR - Kholoud Al-ZainDocument30 pagesOrthopedic History Taking: DR - Kholoud Al-ZainJim Jose AntonyNo ratings yet
- Diagnostic Criteria For Urinary Tract InfectionDocument2 pagesDiagnostic Criteria For Urinary Tract InfectioncandyslibioNo ratings yet
- Hair Disorders and Pigmented Disorders of The SkinDocument8 pagesHair Disorders and Pigmented Disorders of The SkinJim Jose AntonyNo ratings yet
- SampleH&P PDFDocument6 pagesSampleH&P PDFJim Jose AntonyNo ratings yet
- Anatomy of The Nose Nasopharynx and Paranasal Sinuses PDFDocument7 pagesAnatomy of The Nose Nasopharynx and Paranasal Sinuses PDFJim Jose AntonyNo ratings yet
- Pediatric History FormDocument2 pagesPediatric History FormJim Jose AntonyNo ratings yet
- Medicine Annotated Multiple ChoiceDocument20 pagesMedicine Annotated Multiple ChoiceJim Jose AntonyNo ratings yet
- MCQ Questions May 2006Document10 pagesMCQ Questions May 2006Jim Jose AntonyNo ratings yet
- Motor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistDocument36 pagesMotor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistJim Jose Antony100% (1)
- Paranasal SinusesDocument7 pagesParanasal SinusesJim Jose AntonyNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Cross Sectional Purposive Sampling (Checklist) .: Keyword: Phlebitis, Intravenous Medicine Application, Aseptic TechniqueDocument10 pagesCross Sectional Purposive Sampling (Checklist) .: Keyword: Phlebitis, Intravenous Medicine Application, Aseptic TechniqueFebri NgestiutamaNo ratings yet
- LP Askep Keluarga Gouth AthritisDocument50 pagesLP Askep Keluarga Gouth AthritisSeptyari100% (3)
- Seborrehic DermatitisDocument25 pagesSeborrehic DermatitisHallidayNo ratings yet
- The Influence of Cymbopogon Oil (Cymbopogon Nardus L) On Elderly's Rheumatoid Arthritis Pain Intensity ReductionDocument6 pagesThe Influence of Cymbopogon Oil (Cymbopogon Nardus L) On Elderly's Rheumatoid Arthritis Pain Intensity ReductionElsi Nursyahdin MayaranaNo ratings yet
- Kode IcdDocument5 pagesKode IcdNurul FatimahNo ratings yet
- Irritant Contact Dermatitis Dermatitis Kontak Iritan: June 2, 2019Document5 pagesIrritant Contact Dermatitis Dermatitis Kontak Iritan: June 2, 2019YusufNo ratings yet
- ARTHRITISDocument12 pagesARTHRITISram krishna100% (1)
- Icd 10Document3 pagesIcd 10SriHandaryatiNo ratings yet
- Pengaruh Kompres Hangat Menggunakan Jahe Merah Terhadap Penurunan Skala Nyeri Pada Penderita Gout ArthritisDocument6 pagesPengaruh Kompres Hangat Menggunakan Jahe Merah Terhadap Penurunan Skala Nyeri Pada Penderita Gout ArthritisEga MartiNo ratings yet
- Severity Scoring of Atopic Dermatitis Index SCORAD PDFDocument1 pageSeverity Scoring of Atopic Dermatitis Index SCORAD PDFSlamet RihadiNo ratings yet
- Gambaran Faal Paru Pada Pasien Asma Yang Melakukan Senam Asma Dengan Yang Tidak Melakukan Senam Asma Uci Tama Azilla Sri Melati Munir Eka BebasariDocument17 pagesGambaran Faal Paru Pada Pasien Asma Yang Melakukan Senam Asma Dengan Yang Tidak Melakukan Senam Asma Uci Tama Azilla Sri Melati Munir Eka BebasariiqbalNo ratings yet
- Textbook of Dermatology Eczema, Prurigo, Lichenification, and Erithroderma.7Document1 pageTextbook of Dermatology Eczema, Prurigo, Lichenification, and Erithroderma.7fegx_17No ratings yet
- Orbital and Periorbital PhlegmonDocument21 pagesOrbital and Periorbital Phlegmonlulondon1No ratings yet
- Dermatitis and HomoeopathyDocument18 pagesDermatitis and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- T43 Musculoskeletal Infection and Inflammation PTP 0720Document5 pagesT43 Musculoskeletal Infection and Inflammation PTP 0720angela adelantarNo ratings yet
- Dermatitis: DefinitionDocument5 pagesDermatitis: DefinitionSuhas IngaleNo ratings yet
- Episkleritis N Skleritis EditDocument12 pagesEpiskleritis N Skleritis EditAnonymous HgX3mN1oNo ratings yet
- Infl. Bowel DisDocument2 pagesInfl. Bowel DisqwertyNo ratings yet
- EpiscleritisDocument3 pagesEpiscleritisvedorangeliaNo ratings yet
- Classification of Rheumatic DiseasesDocument29 pagesClassification of Rheumatic DiseasesBahaa Shaaban100% (5)
- Prof. DR. Dr. Benny E. Wiryadi, SP - KK (K)Document30 pagesProf. DR. Dr. Benny E. Wiryadi, SP - KK (K)Margaretta WijayantiNo ratings yet
- DR Natsir SPPD KR Painful JointDocument41 pagesDR Natsir SPPD KR Painful JointSITI BINTA MASYKURINNo ratings yet
- Juli 21Document15 pagesJuli 21Asam CemaraNo ratings yet
- Vasculitis StepDocument2 pagesVasculitis Stepcsa yanisis hernandezNo ratings yet
- 450-Article Text-2539-1-10-20200925Document5 pages450-Article Text-2539-1-10-20200925Zefanya Cornelia SimorangkirNo ratings yet
- Nummular EczemaDocument1 pageNummular EczemaCitra AnandiraNo ratings yet
- Approach To The Patient With ArthritisDocument10 pagesApproach To The Patient With ArthritisshosmedNo ratings yet
- Jurnal Seborrhea 2020Document8 pagesJurnal Seborrhea 2020Edom LazarNo ratings yet
- Lap Pelayanan SeptemberDocument12 pagesLap Pelayanan SeptemberJosepb SimarmataNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakalenaarfahNo ratings yet