You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- 6min English Kids at Home PDFDocument5 pages6min English Kids at Home PDFJim Jose AntonyNo ratings yet
- 6min English Electricity PDFDocument5 pages6min English Electricity PDFJim Jose AntonyNo ratings yet
- Acne Vulgaris and Acne Related DisordersDocument12 pagesAcne Vulgaris and Acne Related DisordersJim Jose AntonyNo ratings yet
- Refractive ErrorsDocument7 pagesRefractive ErrorsJim Jose AntonyNo ratings yet
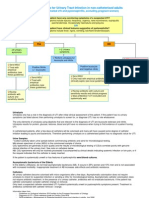
- Urinary Tract Infection in Children: Dr. Alia Al-Ibrahim Consultant Pediatric Nephrology Clinical Assistant ProfessorDocument11 pagesUrinary Tract Infection in Children: Dr. Alia Al-Ibrahim Consultant Pediatric Nephrology Clinical Assistant ProfessorJim Jose AntonyNo ratings yet
- Ocular EmergenciesDocument4 pagesOcular EmergenciesJim Jose AntonyNo ratings yet
- Immunization in Children: Fahad Al ZamilDocument44 pagesImmunization in Children: Fahad Al ZamilJim Jose AntonyNo ratings yet
- India Today 29 June 2020 PDFDocument76 pagesIndia Today 29 June 2020 PDFJim Jose AntonyNo ratings yet
- Dr. Elham Bukhari: Aediatri Nfectious IseaseDocument56 pagesDr. Elham Bukhari: Aediatri Nfectious IseaseJim Jose AntonyNo ratings yet
- Common Cutaneous Infections and InfestationsDocument28 pagesCommon Cutaneous Infections and InfestationsJim Jose AntonyNo ratings yet
- Optha: NeuroDocument13 pagesOptha: NeuroJim Jose AntonyNo ratings yet
- Ortho Team FinalDocument221 pagesOrtho Team FinalJim Jose AntonyNo ratings yet
- Acute Visual LossDocument10 pagesAcute Visual LossJim Jose AntonyNo ratings yet
- Chronic Visual LossDocument7 pagesChronic Visual LossJim Jose AntonyNo ratings yet
- Investigations of Lung DiseasesDocument14 pagesInvestigations of Lung DiseasesJim Jose AntonyNo ratings yet
- COPD and BronchiectasisDocument20 pagesCOPD and BronchiectasisJim Jose AntonyNo ratings yet
- Hair Disorders and Pigmented Skin ConditionsDocument8 pagesHair Disorders and Pigmented Skin ConditionsJim Jose AntonyNo ratings yet
- Pleural EffusionDocument10 pagesPleural EffusionJim Jose Antony100% (1)
- GoutDocument1 pageGoutJim Jose AntonyNo ratings yet
- Diagnostic Criteria For Urinary Tract InfectionDocument2 pagesDiagnostic Criteria For Urinary Tract InfectioncandyslibioNo ratings yet
- Medicine Annotated Multiple ChoiceDocument20 pagesMedicine Annotated Multiple ChoiceJim Jose AntonyNo ratings yet
- Cardiology Disease List PDFDocument139 pagesCardiology Disease List PDFJim Jose AntonyNo ratings yet
- Motor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistDocument36 pagesMotor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistJim Jose Antony100% (1)
- History and Physical Exam of Depressed College StudentDocument6 pagesHistory and Physical Exam of Depressed College StudentJim Jose AntonyNo ratings yet
- MCQ Questions May 2006Document10 pagesMCQ Questions May 2006Jim Jose AntonyNo ratings yet
- Pediatric History FormDocument2 pagesPediatric History FormJim Jose AntonyNo ratings yet
- Orthopedic History Taking: DR - Kholoud Al-ZainDocument30 pagesOrthopedic History Taking: DR - Kholoud Al-ZainJim Jose AntonyNo ratings yet
- Anatomy of The Nose Nasopharynx and Paranasal Sinuses PDFDocument7 pagesAnatomy of The Nose Nasopharynx and Paranasal Sinuses PDFJim Jose AntonyNo ratings yet
- Paranasal SinusesDocument7 pagesParanasal SinusesJim Jose AntonyNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- February 2018 Ophthalmic PearlsDocument3 pagesFebruary 2018 Ophthalmic PearlstiaraleshaNo ratings yet
- Cirrus 6000 - PosterDocument1 pageCirrus 6000 - PosterDim BoyNo ratings yet
- Human Eye NDADocument7 pagesHuman Eye NDAKushal SahaNo ratings yet
- The Secret of The Golden Flower PDFDocument4 pagesThe Secret of The Golden Flower PDFPranavNo ratings yet
- Microeconomics 5th Edition Krugman Solutions ManualDocument35 pagesMicroeconomics 5th Edition Krugman Solutions Manualsintochenge62100% (21)
- Pharmacotherapeutics For Nurse Practitioner Prescribers 3rd Edition Moser Woo Test BankDocument36 pagesPharmacotherapeutics For Nurse Practitioner Prescribers 3rd Edition Moser Woo Test Banksaltinghaughiiphpb100% (26)
- World Sight Day - 8 October 2020Document7 pagesWorld Sight Day - 8 October 2020Times MediaNo ratings yet
- Periodontal Microsurgery-A ReviewDocument4 pagesPeriodontal Microsurgery-A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- How To Reverse Your Cataracts Naturally: 5 Ways To Do It: William BodriDocument39 pagesHow To Reverse Your Cataracts Naturally: 5 Ways To Do It: William Bodrilefty51100% (5)
- 10 Exercises For Speed ReadingDocument6 pages10 Exercises For Speed Readingmanchiraju raj kumarNo ratings yet
- DGCA & EASA Module 9 Human Factors Questions PART-1Document87 pagesDGCA & EASA Module 9 Human Factors Questions PART-1Ravishek Sharma100% (6)
- Direct OphthalmoscopeDocument16 pagesDirect OphthalmoscopeMuhammed AbdulmajeedNo ratings yet
- Report of Vision 2020 IAPB Workshop IndonesiaDocument12 pagesReport of Vision 2020 IAPB Workshop IndonesiaAstidya Miranti100% (1)
- Examining ChildrenDocument31 pagesExamining ChildrenEmmanuel NdukaNo ratings yet
- Uganda Clinical Guidelines Eye Care FinalDocument61 pagesUganda Clinical Guidelines Eye Care FinalSiti Aishah Binti Mazli Hishman100% (2)
- Alexander Technique Improves Vision and Reduces StressDocument22 pagesAlexander Technique Improves Vision and Reduces StressAndra Sukma100% (1)
- Light and Architectural Lighting SystemsDocument17 pagesLight and Architectural Lighting SystemsCrystal Kaye CortezNo ratings yet
- #30 FleshgraftsDocument17 pages#30 FleshgraftsLilith KaneNo ratings yet
- Cataract and Implant Surgery: Dominic Mchugh MD Frcs London, UkDocument33 pagesCataract and Implant Surgery: Dominic Mchugh MD Frcs London, UkVigneshNo ratings yet
- Eye ExaminationDocument9 pagesEye ExaminationFilbert KunardiNo ratings yet
- M1B521614 Ophthalmic Anatomy and PhysiologyDocument1 pageM1B521614 Ophthalmic Anatomy and PhysiologySofina MukhtarNo ratings yet
- SvaDocument32 pagesSvaRameshLoganathanNo ratings yet
- Bio5 1Document7 pagesBio5 1HarmonyChuiNo ratings yet
- 10 Science Imp ch11 2Document6 pages10 Science Imp ch11 2Jagpreet SinghNo ratings yet
- Kowa Ophthalmic Diagnostics KW 2000 BrochureDocument1 pageKowa Ophthalmic Diagnostics KW 2000 BrochureBayu AdhityaNo ratings yet
- Management of Juvenile Glaucoma With TrabeculectomyDocument147 pagesManagement of Juvenile Glaucoma With TrabeculectomyErlinaerlin100% (1)
- Poster Chi2 - Ocular Albinism HKDocument1 pagePoster Chi2 - Ocular Albinism HKyollayusticiaNo ratings yet
- Thoughts On Ocular Dominance-Is It Actually A Preference?: Daniel M. Laby, and David G. KirschenDocument5 pagesThoughts On Ocular Dominance-Is It Actually A Preference?: Daniel M. Laby, and David G. KirschenMaria FernandaNo ratings yet
- Guide to Strabismus Types and ClassificationsDocument65 pagesGuide to Strabismus Types and ClassificationsLavanya MadabushiNo ratings yet
- Seeley's Essential Anaphy Chapter 9 Seeley's Essential Anaphy Chapter 9Document9 pagesSeeley's Essential Anaphy Chapter 9 Seeley's Essential Anaphy Chapter 9Aysha AishaNo ratings yet