You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Radicular Cavity PreparationDocument64 pagesRadicular Cavity PreparationAndrea LawNo ratings yet
- Basic Splinting TechniquesDocument5 pagesBasic Splinting TechniquesAdy KimNo ratings yet
- Unit 2 - TYPES OF RECREATION Part 2Document22 pagesUnit 2 - TYPES OF RECREATION Part 2Reina100% (6)
- Books About GroupsDocument25 pagesBooks About GroupsgerawenceNo ratings yet
- Patellofemoral Final PDFDocument12 pagesPatellofemoral Final PDFdvenumohanNo ratings yet
- Lifestyle Drug & Me-Too Drugs: by Tutor A6 @tutorarbowDocument14 pagesLifestyle Drug & Me-Too Drugs: by Tutor A6 @tutorarbowKeyvan FermitaliansyahNo ratings yet
- Breast Cancer Differential DiagnosesDocument5 pagesBreast Cancer Differential DiagnosesRayhanun MardhatillahNo ratings yet
- Flight 60 Service Manual RevaDocument101 pagesFlight 60 Service Manual RevaMarcel GhidusulNo ratings yet
- Tabela Grifo LaboratoryDocument11 pagesTabela Grifo LaboratoryGRIFO DIVULGA100% (2)
- UT Trauma HandbookDocument49 pagesUT Trauma Handbooksgod34No ratings yet
- Reality TherapyDocument2 pagesReality TherapyAGLDNo ratings yet
- Diagnosis and Management of HyperhidrosisDocument8 pagesDiagnosis and Management of HyperhidrosisLaurence Arcon BanalNo ratings yet
- CKD CHCRTDocument28 pagesCKD CHCRTNurhidayati KeriyunNo ratings yet
- Dialysis Power PointDocument20 pagesDialysis Power PointJor GarciaNo ratings yet
- Movie Characters and Personality DisordersDocument2 pagesMovie Characters and Personality DisordersDanielsenOsman1No ratings yet
- Management of Fear Anxiety PedoDocument21 pagesManagement of Fear Anxiety PedoFourthMolar.comNo ratings yet
- Colorectal CancerDocument23 pagesColorectal Cancerralph_gail100% (1)
- The Differences Between Coaching Mentoring Therapy and Counselling PDFDocument5 pagesThe Differences Between Coaching Mentoring Therapy and Counselling PDFghinaNo ratings yet
- EnglishDocument56 pagesEnglishPankaj SharmaNo ratings yet
- PublicationDocument5 pagesPublicationMahfuzur RNo ratings yet
- ProposalDocument45 pagesProposalJP firmNo ratings yet
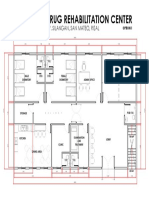
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalDocument1 pageProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonNo ratings yet
- ESC Guidelines for Diagnosis and Treatment of Acute and Chronic Heart FailureDocument61 pagesESC Guidelines for Diagnosis and Treatment of Acute and Chronic Heart FailureSurya ArhNo ratings yet
- CBT of DepressionDocument15 pagesCBT of DepressionRidwan MuttaqinNo ratings yet
- DVT Formation and TreatmentDocument24 pagesDVT Formation and TreatmentdinafiniNo ratings yet
- Endotracheal Tube ETT Insertion IntubationDocument3 pagesEndotracheal Tube ETT Insertion IntubationmochkurniawanNo ratings yet
- Nursing Care PlanDocument26 pagesNursing Care PlanNeil Anthony78% (18)
- Kuliah Dislipidemia UpdateDocument44 pagesKuliah Dislipidemia UpdateYudy Hardiyansah100% (1)
- Higado 1Document86 pagesHigado 1Carlos CuadrosNo ratings yet
- Oncology ExamDocument5 pagesOncology ExamRabeed MohammedNo ratings yet