You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Nature of Philosophy and Its ObjectsDocument9 pagesThe Nature of Philosophy and Its Objectsaugustine abellanaNo ratings yet
- Synopsis: in Order To Decrease Cross Sectional Area of Structural Members, Ultra High StrengthDocument16 pagesSynopsis: in Order To Decrease Cross Sectional Area of Structural Members, Ultra High StrengthHector Alberto Garcia LopezNo ratings yet
- 0620 Chemistry: MARK SCHEME For The March 2015 SeriesDocument6 pages0620 Chemistry: MARK SCHEME For The March 2015 SeriesDark GreenNo ratings yet
- Lab 2 Centrifugal PumpsDocument29 pagesLab 2 Centrifugal PumpslalelaNo ratings yet
- Newtons CowsDocument9 pagesNewtons CowsLawrence Lim Ah KowNo ratings yet
- Power Electronics - MITDocument210 pagesPower Electronics - MITVasco RodriguesNo ratings yet
- Cambridge O Level: PHYSICS 5054/03Document16 pagesCambridge O Level: PHYSICS 5054/03Titan XosmosNo ratings yet
- ALGEBRA 1B Solving Quadratic EquationsDocument2 pagesALGEBRA 1B Solving Quadratic EquationsMaurizio FanniNo ratings yet
- Physical symbol system hypothesis: An overviewDocument5 pagesPhysical symbol system hypothesis: An overviewKostasBaliotisNo ratings yet
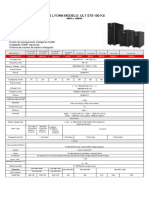
- Ups Lyonn Modelo: Ult St5-100 KS: 10KVA A 120KVADocument1 pageUps Lyonn Modelo: Ult St5-100 KS: 10KVA A 120KVASebastian Matias CruzNo ratings yet
- (Altium Tutorial) PCB Symbol Naming ConventionDocument7 pages(Altium Tutorial) PCB Symbol Naming ConventionDefne AktemizNo ratings yet
- Heliosit OrthodonticDocument20 pagesHeliosit OrthodonticAndhika Galih PrasetyoNo ratings yet
- Chapter 2 - Exercises - Econometrics2Document2 pagesChapter 2 - Exercises - Econometrics2Mai AnhNo ratings yet
- Understanding the Strength and Limitations of DES EncryptionDocument32 pagesUnderstanding the Strength and Limitations of DES EncryptionArya KumariNo ratings yet
- Hitachi ZW550Document12 pagesHitachi ZW550ForomaquinasNo ratings yet
- Coreldraw 12 Hotkeys - Keyboard ShortcutsDocument6 pagesCoreldraw 12 Hotkeys - Keyboard ShortcutsRais AhmadNo ratings yet
- Surge Current Protection Using SuperconductorDocument25 pagesSurge Current Protection Using SuperconductorAbhishek Walter PaulNo ratings yet
- Solutions: Rise Desnita, M.Si., AptDocument41 pagesSolutions: Rise Desnita, M.Si., Aptdeput_rprNo ratings yet
- Chapter 3 - Methods of Analysis: N N N N A A A ADocument15 pagesChapter 3 - Methods of Analysis: N N N N A A A AvampakkNo ratings yet
- DPWH Design Assessment ChecklistDocument18 pagesDPWH Design Assessment ChecklistGeovanni DumpasanNo ratings yet
- Power Max India PVT LTD Extra Work Done at VMW Shed WorksDocument4 pagesPower Max India PVT LTD Extra Work Done at VMW Shed WorksparthaNo ratings yet
- Esolutions Manual - Powered by CogneroDocument31 pagesEsolutions Manual - Powered by CogneroAll About MusicNo ratings yet
- 93C66 Microwire EepromDocument13 pages93C66 Microwire EepromadrianramonNo ratings yet
- American Journal of Sociology Volume 46 Issue 3 1940 (Doi 10.2307/2769572) C. Wright Mills - Methodological Consequences of The Sociology of KnowledgeDocument16 pagesAmerican Journal of Sociology Volume 46 Issue 3 1940 (Doi 10.2307/2769572) C. Wright Mills - Methodological Consequences of The Sociology of KnowledgeBobi BadarevskiNo ratings yet
- CSC4212 Lecture 3 - 3D Viewing - Projection TransformationDocument31 pagesCSC4212 Lecture 3 - 3D Viewing - Projection TransformationAhmad AbbaNo ratings yet
- HP LaserJet 5P - 6P Service Manual (Proper)Document116 pagesHP LaserJet 5P - 6P Service Manual (Proper)maroudasp100% (1)
- Straight Line MotionDocument12 pagesStraight Line MotionMZWAANo ratings yet
- SOP's For All Digital Marketing ActivitesDocument3 pagesSOP's For All Digital Marketing ActivitesSavijeet Singh50% (2)
- UDP Control and Monitoring With PIC Microcontroller - StudentCompanion PDFDocument14 pagesUDP Control and Monitoring With PIC Microcontroller - StudentCompanion PDFVport PortNo ratings yet
- Vendor Information Vishay BLH Handbook TC0013 Solutions For Process Weighing and Force Measurement Electronic Weigh SystemsDocument59 pagesVendor Information Vishay BLH Handbook TC0013 Solutions For Process Weighing and Force Measurement Electronic Weigh SystemsAndrew JacksonNo ratings yet