You might also like
- 1 s2.0 S1877042816305237 Main PDFDocument9 pages1 s2.0 S1877042816305237 Main PDFsumit6singhNo ratings yet
- PCR IT RatioDocument5 pagesPCR IT RatioAgus WijayaNo ratings yet
- I Made You Mine by Futen22Document514 pagesI Made You Mine by Futen22Indra T BudiantoNo ratings yet
- 3 2007 Benign Proliferative Epithelial Disorders of The Breast A Review of The Epidemiologic EvidenceDocument13 pages3 2007 Benign Proliferative Epithelial Disorders of The Breast A Review of The Epidemiologic EvidenceIndra T BudiantoNo ratings yet
- 21 2009 Extracorporeal Membrane Oxygenation ForDocument8 pages21 2009 Extracorporeal Membrane Oxygenation ForIndra T BudiantoNo ratings yet
- 2003 Management of Hypertensive Emergencies PDFDocument4 pages2003 Management of Hypertensive Emergencies PDFIndra T BudiantoNo ratings yet
- Significance of Hematological Scoring System (HSS)Document4 pagesSignificance of Hematological Scoring System (HSS)Indra T BudiantoNo ratings yet
- Definitions of Bloodstream Infection in The.11Document5 pagesDefinitions of Bloodstream Infection in The.11Indra T BudiantoNo ratings yet
- 16 2012 Magnesium Sulphate Versus Sildenafil in The Treatment ofDocument7 pages16 2012 Magnesium Sulphate Versus Sildenafil in The Treatment ofIndra T BudiantoNo ratings yet
- 2012 Extubation of The Difficult Airway An Algorithmic Approach PDFDocument8 pages2012 Extubation of The Difficult Airway An Algorithmic Approach PDFIndra T BudiantoNo ratings yet
- 19 2015 Weaning of Inhaled Nitric OxideDocument11 pages19 2015 Weaning of Inhaled Nitric OxideIndra T BudiantoNo ratings yet
- 2014 Ambulatory Blood Pressure Monitoring in ChildrenDocument3 pages2014 Ambulatory Blood Pressure Monitoring in ChildrenIndra T BudiantoNo ratings yet
- 2015 Vestibular Disorders in Children WithDocument9 pages2015 Vestibular Disorders in Children WithIndra T BudiantoNo ratings yet
- Manegament VA in ObstetriciaDocument5 pagesManegament VA in ObstetriciaLeandro Gonzalez MorenoNo ratings yet
- 2005 Cannot Intubate-Cannot Ventilate and Difficult IntubationDocument8 pages2005 Cannot Intubate-Cannot Ventilate and Difficult IntubationIndra T BudiantoNo ratings yet
- Hypovolemic Shock Guidelines PDFDocument8 pagesHypovolemic Shock Guidelines PDFAloysia Catur WidiNo ratings yet
- Lembar Jawaban PORTRAITDocument1 pageLembar Jawaban PORTRAITIndra T BudiantoNo ratings yet
- 9 2013 Severe Postpartum Hemorrhage From Uterine Atony A Multicentric Study PDFDocument7 pages9 2013 Severe Postpartum Hemorrhage From Uterine Atony A Multicentric Study PDFIndra T BudiantoNo ratings yet
- LG 2013 04 Association BetweenDocument6 pagesLG 2013 04 Association BetweenAbdalmonem AlbazNo ratings yet
- Complications of Endotracheal Intubation and Other Airway Management ProceduresDocument11 pagesComplications of Endotracheal Intubation and Other Airway Management ProceduresSuresh Kumar100% (1)
- 23 2015 Maternal Morbidity For Vaginal and Cesarean Deliveries, According To Previous Cesarean History New Data From The Birth Certificate, 2013 PDFDocument14 pages23 2015 Maternal Morbidity For Vaginal and Cesarean Deliveries, According To Previous Cesarean History New Data From The Birth Certificate, 2013 PDFIndra T BudiantoNo ratings yet
- 1996 Diagnosis of Cytomegalovirus Infection in Pediatric Menetrier'sDocument2 pages1996 Diagnosis of Cytomegalovirus Infection in Pediatric Menetrier'sIndra T BudiantoNo ratings yet
- 2001 Assessment of Vitamin B-6 Status in Young Women Consuming ADocument11 pages2001 Assessment of Vitamin B-6 Status in Young Women Consuming AIndra T BudiantoNo ratings yet
- 12 2002 Patterns of Multiple Recurrences of SuperficialDocument9 pages12 2002 Patterns of Multiple Recurrences of SuperficialIndra T BudiantoNo ratings yet
- 7 2015 Guidelines On Muscle-Invasive and Metastatic Bladder Cancer PDFDocument60 pages7 2015 Guidelines On Muscle-Invasive and Metastatic Bladder Cancer PDFIndra T BudiantoNo ratings yet
- 2002 Conventional Treatments For Ankylosing Spondylitis PDFDocument12 pages2002 Conventional Treatments For Ankylosing Spondylitis PDFIndra T BudiantoNo ratings yet
- 2000 Gambaran Perubahan Status Gizi Anak Balita Gizi Buruk PDFDocument7 pages2000 Gambaran Perubahan Status Gizi Anak Balita Gizi Buruk PDFIndra T BudiantoNo ratings yet
- 2002 Conventional Treatments For Ankylosing Spondylitis PDFDocument12 pages2002 Conventional Treatments For Ankylosing Spondylitis PDFIndra T BudiantoNo ratings yet
- Definitions of Bloodstream Infection in The.11Document5 pagesDefinitions of Bloodstream Infection in The.11Indra T BudiantoNo ratings yet
- 2016 Laryngeal Injury in NeonateDocument4 pages2016 Laryngeal Injury in NeonateIndra T BudiantoNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Diseases and Immunity: Defence Against MicrobesDocument55 pagesDiseases and Immunity: Defence Against MicrobesIvan Prasetya100% (1)
- Bulgarian Split Squat Lateral: Lateral LungeDocument47 pagesBulgarian Split Squat Lateral: Lateral LungeZac Brouillette100% (10)
- Anatomy of The Skull & BrainDocument61 pagesAnatomy of The Skull & BrainMirza SullivanNo ratings yet
- Electric Eels Use High-Voltage To Track Fast-MovinDocument6 pagesElectric Eels Use High-Voltage To Track Fast-MovinTatsumaki TornadoNo ratings yet
- Chapter 2 - PoriferaDocument23 pagesChapter 2 - PoriferaHeilene Ethel AngcayaNo ratings yet
- Biopharmaceutics and Pharmacokinetics: Pharmacy Board Review Module 4Document73 pagesBiopharmaceutics and Pharmacokinetics: Pharmacy Board Review Module 4Kate EvangelistaNo ratings yet
- Bci - 3303 - User ManualDocument52 pagesBci - 3303 - User ManualNuno Freitas BastosNo ratings yet
- Anatomy and Physiology of The Larynx Copy 2Document61 pagesAnatomy and Physiology of The Larynx Copy 2Karimah SahabNo ratings yet
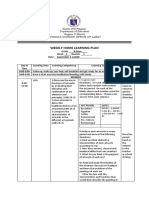
- Weekly Home Learning Plan: Department of EducationDocument19 pagesWeekly Home Learning Plan: Department of EducationMaya CondeNo ratings yet
- Metabolic Reprogramming Due To Hypoxia in Pancreatic Can - 2021 - BiomedicineDocument14 pagesMetabolic Reprogramming Due To Hypoxia in Pancreatic Can - 2021 - BiomedicineAkhmad BajuriNo ratings yet
- BiochemDocument5 pagesBiochemHarvey Mher RarangNo ratings yet
- GR 173259Document11 pagesGR 173259Anonymous wDganZNo ratings yet
- Open Cloze IDocument2 pagesOpen Cloze IRadu BortesNo ratings yet
- The Role of Collagen in Bone StrengthDocument19 pagesThe Role of Collagen in Bone StrengthClaudia AndreeaNo ratings yet
- The Menstrual Cycle PDFDocument6 pagesThe Menstrual Cycle PDFPerry Sin100% (1)
- Alberts-Chapter 11-Membrane TransportDocument44 pagesAlberts-Chapter 11-Membrane TransportMayra SanchezNo ratings yet
- Measurement of Enolase Activity in Cell LysatesDocument10 pagesMeasurement of Enolase Activity in Cell LysatesClinton LunaNo ratings yet
- Material Mini NetterDocument11 pagesMaterial Mini NetterVALENTINA ALBORNOZ BASTÍASNo ratings yet
- Interstitial Vs AlveolarDocument17 pagesInterstitial Vs AlveolarEdwin DarmawanNo ratings yet
- Articular Neurophysiology: Presented by - Yogesh VyasDocument15 pagesArticular Neurophysiology: Presented by - Yogesh VyasvictoryvelavaNo ratings yet
- The Failing Heart-An Engine Out of FuelDocument12 pagesThe Failing Heart-An Engine Out of FuelJorge Leonardo BedoyaNo ratings yet
- Overview of Anatomy and Physiology Lesson 1Document28 pagesOverview of Anatomy and Physiology Lesson 1Vincent Dajao CimafrancaNo ratings yet
- Delayed Awakening From AnaesthesiaDocument3 pagesDelayed Awakening From AnaesthesiaSenthooran ArudshivsmNo ratings yet
- BT01110300041275232 RLS PDFDocument14 pagesBT01110300041275232 RLS PDFnk2k10No ratings yet
- 0038 Foldrajz Palaeontologyda PDFDocument54 pages0038 Foldrajz Palaeontologyda PDFRamón F. Zapata Sánchez100% (1)
- HHS Public Access: The Role of Oxidative Stress in Anxiety Disorder: Cause or Consequence?Document23 pagesHHS Public Access: The Role of Oxidative Stress in Anxiety Disorder: Cause or Consequence?yenny handayani sihiteNo ratings yet
- Lesson Plan Heart DiseaseDocument3 pagesLesson Plan Heart Diseaseapi-417867384No ratings yet
- Inflammation and Mental HealthDocument41 pagesInflammation and Mental HealthanindyaguptaNo ratings yet
- The Blalock and Taussig Shunt Revisited: Review ArticleDocument8 pagesThe Blalock and Taussig Shunt Revisited: Review ArticlearwitarahayuNo ratings yet
- Adding An "R" in The "DOPE" Mnemonic For Ventilator TroubleshootingDocument1 pageAdding An "R" in The "DOPE" Mnemonic For Ventilator TroubleshootingkelvinaNo ratings yet