You might also like
- Muslo Posterior EcoDocument9 pagesMuslo Posterior EcoGabriela SerraNo ratings yet
- Knee Pain and The Infrapatellar Branch of The Saphenous: NerveDocument3 pagesKnee Pain and The Infrapatellar Branch of The Saphenous: NervefostizzNo ratings yet
- Aime201704040 M162367Document29 pagesAime201704040 M162367Ziggy GonNo ratings yet
- Ox Efect Os Biologic OsDocument7 pagesOx Efect Os Biologic OsfostizzNo ratings yet
- Sdre Gluteo ProfundoDocument6 pagesSdre Gluteo ProfundofostizzNo ratings yet
- ONDAS CHOQUE EpicondilitisDocument6 pagesONDAS CHOQUE EpicondilitisfostizzNo ratings yet
- ONDAS DE CHOQUE Tendinitis PatellaDocument5 pagesONDAS DE CHOQUE Tendinitis PatellafostizzNo ratings yet
- Vibe Fersum Et Al 2012 Appendix 1 at 290912 2 PDFDocument1 pageVibe Fersum Et Al 2012 Appendix 1 at 290912 2 PDFfostizzNo ratings yet
- Knee Pain and The Infrapatellar Branch of The Saphenous: NerveDocument3 pagesKnee Pain and The Infrapatellar Branch of The Saphenous: NervefostizzNo ratings yet
- Guia Nice Lumbalgia PDFDocument25 pagesGuia Nice Lumbalgia PDFfostizzNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Creating Rapid Prototype Metal CastingsDocument10 pagesCreating Rapid Prototype Metal CastingsShri JalihalNo ratings yet
- Unit 4: A World of Ideas: Learning CompassDocument3 pagesUnit 4: A World of Ideas: Learning CompassRica Mae Lepiten MendiolaNo ratings yet
- Paulson 2007 Year End Report Earns Nearly 600Document16 pagesPaulson 2007 Year End Report Earns Nearly 600Tunaljit ChoudhuryNo ratings yet
- Training Prospectus 2020 WebDocument89 pagesTraining Prospectus 2020 Webamila_vithanageNo ratings yet
- Green Ecobuses Run On This Route.: BusesDocument6 pagesGreen Ecobuses Run On This Route.: BusesLuis DíazNo ratings yet
- Section 2 in The Forest (Conservation) Act, 1980Document1 pageSection 2 in The Forest (Conservation) Act, 1980amit singhNo ratings yet
- 244256-Exabeam Security Content in The Legacy Structure-Pdf-EnDocument142 pages244256-Exabeam Security Content in The Legacy Structure-Pdf-EnYoussef MohamedNo ratings yet
- Module 1 (Social Innovation)Document7 pagesModule 1 (Social Innovation)Marinette Medrano50% (2)
- 2008 Application FormDocument12 pages2008 Application FormVishal PonugotiNo ratings yet
- Destruction FormDocument2 pagesDestruction FormHanabishi RekkaNo ratings yet
- Electricity BillDocument1 pageElectricity BillSushila SinghNo ratings yet
- Resume DaniellaAmatoDocument2 pagesResume DaniellaAmatoDaniellaNo ratings yet
- 3.1.2 Cable FPLR 2X18 AwgDocument3 pages3.1.2 Cable FPLR 2X18 Awgluis rios granadosNo ratings yet
- Rheomix 141Document5 pagesRheomix 141Haresh BhavnaniNo ratings yet
- MU0017 Talent ManagementDocument12 pagesMU0017 Talent ManagementDr. Smita ChoudharyNo ratings yet
- Integrated Building Management Platform for Security, Maintenance and Energy EfficiencyDocument8 pagesIntegrated Building Management Platform for Security, Maintenance and Energy EfficiencyRajesh RajendranNo ratings yet
- Efectele Crizei Economice Asupra Politicilor Pietei Muncii Din RomaniaDocument24 pagesEfectele Crizei Economice Asupra Politicilor Pietei Muncii Din Romaniacristian_incaltarauNo ratings yet
- Nikita Project 01-06-2016Document38 pagesNikita Project 01-06-2016Shobhit GoswamiNo ratings yet
- Pabahay Bonanza: Philippine National Bank As of September 30, 2009Document80 pagesPabahay Bonanza: Philippine National Bank As of September 30, 2009ramonlucas700No ratings yet
- Less Than a Decade to Avoid Catastrophic Climate ChangeDocument1 pageLess Than a Decade to Avoid Catastrophic Climate ChangeXie YuJiaNo ratings yet
- E.R. Hooton, Tom Cooper - Desert Storm - Volume 2 - Operation Desert Storm and The Coalition Liberation of Kuwait 1991 (Middle East@War) (2021, Helion and CompanyDocument82 pagesE.R. Hooton, Tom Cooper - Desert Storm - Volume 2 - Operation Desert Storm and The Coalition Liberation of Kuwait 1991 (Middle East@War) (2021, Helion and Companydubie dubs100% (5)
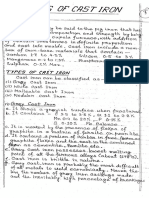
- Welding of Cast IronDocument10 pagesWelding of Cast IronKrishnendu RouthNo ratings yet
- Javacore 20100918 202221 6164 0003Document44 pagesJavacore 20100918 202221 6164 0003actmon123No ratings yet
- Duratone eDocument1 pageDuratone eandreinalicNo ratings yet
- 2022 Semester 2 Letter To Parents - FinalDocument7 pages2022 Semester 2 Letter To Parents - FinalRomanceforpianoNo ratings yet
- Project On SamsungDocument39 pagesProject On SamsungAbbas0% (1)
- Sequence 2: Greet and Seat The GuestDocument3 pagesSequence 2: Greet and Seat The GuestNguyễn Ngọc TrâmNo ratings yet
- Interpretation 1Document17 pagesInterpretation 1ysunnyNo ratings yet
- Evoked PotentialsDocument49 pagesEvoked PotentialsparuNo ratings yet
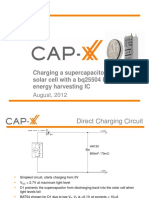
- 1208 CAP XX Charging A Supercapacitor From A Solar Cell PDFDocument12 pages1208 CAP XX Charging A Supercapacitor From A Solar Cell PDFmehralsmenschNo ratings yet