You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- County Draft Strategic Plan PDFDocument107 pagesCounty Draft Strategic Plan PDFDavid SonoiyaNo ratings yet
- First Aid - CPR - AED Participant's ManualDocument196 pagesFirst Aid - CPR - AED Participant's Manualadamiam100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- 0742557057WorldHistory PDFDocument257 pages0742557057WorldHistory PDFMahdi Rezaeian100% (5)
- Pranic Healing Patient Record FormDocument6 pagesPranic Healing Patient Record FormGuida Lourenco100% (2)
- Homosexuality and HopeDocument31 pagesHomosexuality and HopeKernyuy Leonard MbiydzenyuyNo ratings yet
- On The MiasmsDocument5 pagesOn The Miasmsisadore100% (7)
- Communicable Nursing - LecturervDocument329 pagesCommunicable Nursing - LecturervCarl WaletNo ratings yet
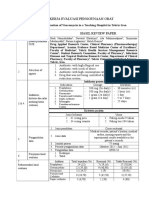
- Review Jurnal VankomisinDocument2 pagesReview Jurnal VankomisinNafiahEmaSuryaniNo ratings yet
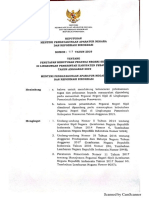
- Formasi CPNS - PESAWARAN2019 PDFDocument30 pagesFormasi CPNS - PESAWARAN2019 PDFNafiahEmaSuryaniNo ratings yet
- Nausea and Vomiting: NCCN Guidelines For PatientsDocument46 pagesNausea and Vomiting: NCCN Guidelines For Patientsmuhamad anwariNo ratings yet
- Colon Cancer PDFDocument88 pagesColon Cancer PDFGemma GarciaNo ratings yet
- Tugas Bu DaniaDocument12 pagesTugas Bu DaniaNafiahEmaSuryaniNo ratings yet
- Acute Diare WHO 2005Document50 pagesAcute Diare WHO 2005Boby Abdul RahmanNo ratings yet
- Management of Acne Guidelines Jan 2015Document4 pagesManagement of Acne Guidelines Jan 2015NafiahEmaSuryaniNo ratings yet
- Nafiah Ema, Nadya Amalia, Wahyu Tirta - FKKBDocument5 pagesNafiah Ema, Nadya Amalia, Wahyu Tirta - FKKBNafiahEmaSuryaniNo ratings yet
- Tugas Bu DaniaDocument12 pagesTugas Bu DaniaNafiahEmaSuryaniNo ratings yet
- Topical AntibioticsDocument2 pagesTopical AntibioticsMusfirah HattaNo ratings yet
- Dextromethorphan and Codeine Objective AssessmentDocument10 pagesDextromethorphan and Codeine Objective AssessmentNafiahEmaSuryaniNo ratings yet
- Tips Writing2013 - DyDocument31 pagesTips Writing2013 - DyNafiahEmaSuryaniNo ratings yet
- Form Critical AppraisalDocument2 pagesForm Critical AppraisalNafiahEmaSuryaniNo ratings yet
- Lam Gambar Fts p3Document3 pagesLam Gambar Fts p3NafiahEmaSuryaniNo ratings yet
- Tugas1 Nafiah Ema Suryani - 1400023171 - VBDocument29 pagesTugas1 Nafiah Ema Suryani - 1400023171 - VBNafiahEmaSuryaniNo ratings yet
- Mucoadhesive PDFDocument9 pagesMucoadhesive PDFNafiahEmaSuryaniNo ratings yet
- IniDocument1 pageIniNafiahEmaSuryaniNo ratings yet
- Tugas 2 (Nafiah Ema Suryani-1400023171 - VB)Document4 pagesTugas 2 (Nafiah Ema Suryani-1400023171 - VB)NafiahEmaSuryaniNo ratings yet
- Analisis Darah Ke 2Document15 pagesAnalisis Darah Ke 2NafiahEmaSuryaniNo ratings yet
- Management of The Patient With HIV DeseaseDocument34 pagesManagement of The Patient With HIV DeseaseTeresa MontesNo ratings yet
- Indicators For MCDocument52 pagesIndicators For MCFinch OdhiamboNo ratings yet
- Tugas Individu Kep KomunitasDocument10 pagesTugas Individu Kep KomunitasMeilissaNo ratings yet
- Vol. 2, Issue 12 - March 19, 2010Document48 pagesVol. 2, Issue 12 - March 19, 2010BladeNo ratings yet
- ThesisDocument23 pagesThesisAnushika AgarwalNo ratings yet
- Labor Influx - KS-05-Excel FileDocument6 pagesLabor Influx - KS-05-Excel FileNatarajan SaravananNo ratings yet
- Assessment of Condom Use For Prevention of Hiv/Aids Among Jimma University Students, Jimmatown, South West EthiopiaDocument42 pagesAssessment of Condom Use For Prevention of Hiv/Aids Among Jimma University Students, Jimmatown, South West EthiopiaFitalaBokaNo ratings yet
- Why Education Matters 11 04 09Document4 pagesWhy Education Matters 11 04 09api-273621685No ratings yet
- Government of Nunavut EHB Policy GuidelinesDocument5 pagesGovernment of Nunavut EHB Policy GuidelinesNunatsiaqNewsNo ratings yet
- Acmc AnswersDocument21 pagesAcmc AnswersAjay IyerNo ratings yet
- PROJECT PROPOSAL FOR THE VehackleDocument5 pagesPROJECT PROPOSAL FOR THE VehackleKalayu KirosNo ratings yet
- Focused Antenatal Care (FANC) : ©Moh-Drh/Domc/Nltp/JhpiegoDocument64 pagesFocused Antenatal Care (FANC) : ©Moh-Drh/Domc/Nltp/Jhpiegodwi handayaniNo ratings yet
- TM2 - K37 - Eye Disorders Due To Tropical DiseasesDocument86 pagesTM2 - K37 - Eye Disorders Due To Tropical DiseasesedelinNo ratings yet
- Mod Is A 27112013Document8 pagesMod Is A 27112013Garankuwa HiphopCommiteeNo ratings yet
- Social Sector Initiatives and GovernmentDocument9 pagesSocial Sector Initiatives and GovernmentChristopher TaylorNo ratings yet
- Methods of Paragraph DevelopmentDocument10 pagesMethods of Paragraph DevelopmentFrancis B. Tatel100% (1)
- GOS CMAM IC Mod1 Introduction Nov2011Document29 pagesGOS CMAM IC Mod1 Introduction Nov2011Nensy AnggrainyNo ratings yet
- Janeway's Immunobiology ReviewDocument2 pagesJaneway's Immunobiology ReviewPhillip McMullenNo ratings yet
- AO No. 2007-0025 PEME For Seafarers Related Documents PDFDocument26 pagesAO No. 2007-0025 PEME For Seafarers Related Documents PDFmariaNo ratings yet
- List of AbbreviationsDocument3 pagesList of AbbreviationsNeha SharmaNo ratings yet
- Health and Wellness Calendar 2020Document1 pageHealth and Wellness Calendar 2020CHARMAINE ACEVEDONo ratings yet
- Cordia Viral MeningitisDocument7 pagesCordia Viral MeningitisAyuagung Chandra Maha DewiNo ratings yet
- ZIM Resources CaregivermanualDocument84 pagesZIM Resources CaregivermanualJoseph Ajayi FAYOMINo ratings yet