You might also like
- Introduction To Hormone-Induced Spawning of Fish: Southern Regional Aquaculture CenterDocument4 pagesIntroduction To Hormone-Induced Spawning of Fish: Southern Regional Aquaculture CenterAnand ChauhanNo ratings yet
- Mechanical-Engineering Gate2016.InfoDocument3 pagesMechanical-Engineering Gate2016.InfoHenryNo ratings yet
- A Seminar Report On Job and Marginal CostingDocument5 pagesA Seminar Report On Job and Marginal CostingAnand ChauhanNo ratings yet
- SSC MTS Exam Paper 2016 14 May 1st ShiftDocument16 pagesSSC MTS Exam Paper 2016 14 May 1st ShiftAnand ChauhanNo ratings yet
- The WindlassDocument7 pagesThe WindlassAnand ChauhanNo ratings yet
- HookDocument5 pagesHookAlwiAlHaddadNo ratings yet
- Energy Conservation in PumpsDocument28 pagesEnergy Conservation in PumpsAnand Chauhan100% (1)
- 2 A Davit CalculationDocument30 pages2 A Davit CalculationKarina RoquelNo ratings yet
- V3 I 104Document21 pagesV3 I 104chethanNo ratings yet
- Srisailam Hydroelectric Power Plant, Andhra Pradesh: Submitted By: Chauhan Anand Umashankar ROLL NO:23 (A)Document6 pagesSrisailam Hydroelectric Power Plant, Andhra Pradesh: Submitted By: Chauhan Anand Umashankar ROLL NO:23 (A)Anand ChauhanNo ratings yet
- Case Study On Application of CadDocument9 pagesCase Study On Application of CadAnand ChauhanNo ratings yet
- Case Study On Application of CadDocument9 pagesCase Study On Application of CadAnand ChauhanNo ratings yet
- Case Study On Application of CadDocument9 pagesCase Study On Application of CadAnand ChauhanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- PLSQL - 5 - 6 - Brayan Ferney Perez Moreno PDFDocument5 pagesPLSQL - 5 - 6 - Brayan Ferney Perez Moreno PDFBryan PerezNo ratings yet
- Choong Yik Son V Majlis Peguam MalaysiaDocument5 pagesChoong Yik Son V Majlis Peguam MalaysiaNUR INSYIRAH ZAININo ratings yet
- Kiambu Policy On Shipment ContainersDocument12 pagesKiambu Policy On Shipment Containersmusiomi2005No ratings yet
- XJ550 Parts ManualDocument121 pagesXJ550 Parts Manualjuan2610100% (5)
- Readme Simocrane Basic Technology v30 PDFDocument4 pagesReadme Simocrane Basic Technology v30 PDFRafaelNo ratings yet
- Case Study Biomaterials Selection For A Joint ReplacementDocument8 pagesCase Study Biomaterials Selection For A Joint ReplacementBjarne Van haegenbergNo ratings yet
- Five Model Intragroup Conflict ManagemantDocument22 pagesFive Model Intragroup Conflict ManagemantmarsNo ratings yet
- OpenStack Installation Guide For (RHEL, CentOS, Fedora)Document140 pagesOpenStack Installation Guide For (RHEL, CentOS, Fedora)kinamedebo100% (1)
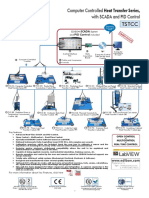
- Computer Controlled Heat Transfer Series SCADA PIDDocument30 pagesComputer Controlled Heat Transfer Series SCADA PIDAli HadiNo ratings yet
- Cosmetic Stability TestingDocument10 pagesCosmetic Stability Testingshivampharma100% (3)
- Chapter 76 - Engine Controls: BHT-206L4-MM-9Document22 pagesChapter 76 - Engine Controls: BHT-206L4-MM-9Raisa RabeyaNo ratings yet
- Vapor Sensor: Installation GuideDocument12 pagesVapor Sensor: Installation GuideShalvaTavdgiridzeNo ratings yet
- (Ye-Tm) Thread Mills PDFDocument12 pages(Ye-Tm) Thread Mills PDFdavidNo ratings yet
- Romac Flanged Couplings for Water and Sewer PipesDocument3 pagesRomac Flanged Couplings for Water and Sewer PipesAl JameelNo ratings yet
- Delivering Success Tesco Case Study On BSCDocument4 pagesDelivering Success Tesco Case Study On BSCWenuri KasturiarachchiNo ratings yet
- Verification of Hook Element in Midas GenDocument3 pagesVerification of Hook Element in Midas GenSASHIN ServiSoftNo ratings yet
- CMBS World - Reremic PhenomenonDocument14 pagesCMBS World - Reremic PhenomenonykkwonNo ratings yet
- Cambridge English For The Media Intermediate Students Book With Audio CD Frontmatter PDFDocument5 pagesCambridge English For The Media Intermediate Students Book With Audio CD Frontmatter PDFBrenda Funes67% (3)
- Summary of Sales Report: Dranix Distributor IncDocument6 pagesSummary of Sales Report: Dranix Distributor Incshipmonk7No ratings yet
- Machine Coverage and Area DetrminationDocument4 pagesMachine Coverage and Area DetrminationMaria Lourdes samontinaNo ratings yet
- High-Voltage Fuse-LinksDocument11 pagesHigh-Voltage Fuse-LinksSatheesh Kumar NatarajanNo ratings yet
- Fri Chiks Marketing Mix and Swot AnalysisDocument22 pagesFri Chiks Marketing Mix and Swot Analysisahsanparveen100% (1)
- Solution Chapter 15Document32 pagesSolution Chapter 15xxxxxxxxx75% (4)
- FACTORS Affecting The Entrepreneurial DynamicsDocument4 pagesFACTORS Affecting The Entrepreneurial DynamicsAzraNo ratings yet
- Ga F2a55m S1Document31 pagesGa F2a55m S1Kleber CostaNo ratings yet
- P2E ProfileDocument10 pagesP2E Profilepr1041No ratings yet
- Chapman, J. C. and Gaydarska, B. I. (2006) 'Parts and Wholes. Fragmentation in Prehistoric Conte XTDocument245 pagesChapman, J. C. and Gaydarska, B. I. (2006) 'Parts and Wholes. Fragmentation in Prehistoric Conte XTSetsuna NicoNo ratings yet
- Proof of Stock OwnershipDocument5 pagesProof of Stock OwnershipSebastian GarciaNo ratings yet
- Magnetic Separator GuideDocument31 pagesMagnetic Separator GuideMNButt100% (1)
- OSV Part 4Document664 pagesOSV Part 4devbsl123No ratings yet