You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- EgyptDocument1 pageEgyptMuhammed HunaisNo ratings yet
- Kmno4 0Document1 pageKmno4 0Muhammed HunaisNo ratings yet
- Pipette Calibration 4-10-09Document7 pagesPipette Calibration 4-10-09Muhammed HunaisNo ratings yet
- Manual On Standard Operation Procedures, Sample Collection and Reference Ranges For Clinical ChemistryDocument103 pagesManual On Standard Operation Procedures, Sample Collection and Reference Ranges For Clinical ChemistryMuhammed Hunais83% (18)
- Guidelines For Maintenance of Equipment in A Clinical Chemistry LaboratoryDocument104 pagesGuidelines For Maintenance of Equipment in A Clinical Chemistry LaboratoryMuhammed Hunais83% (6)
- DENGUE in Tamil LanguageDocument2 pagesDENGUE in Tamil LanguageMuhammed Hunais100% (9)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- How To Concieve A BoyDocument32 pagesHow To Concieve A Boyrelativelabs2075No ratings yet
- Transgenics For Abiotic StressDocument46 pagesTransgenics For Abiotic StressAmit BallaniNo ratings yet
- Atika School-5172016- Biology Form 2Document14 pagesAtika School-5172016- Biology Form 2DenisNo ratings yet
- W. James Kent - BLAT-The BLAST-Like Alignment ToolDocument10 pagesW. James Kent - BLAT-The BLAST-Like Alignment ToolYopghm698No ratings yet
- Bio Practicals 2022-23Document31 pagesBio Practicals 2022-23Aman AaryanNo ratings yet
- Click Here for Taxonomy Questions and AnswersDocument3 pagesClick Here for Taxonomy Questions and AnswersSylvester Asare100% (1)
- Anti Diabetik A Oral: Dr. Theodorus, Mmedsc Staf Bagian Farmakologi FK UnsriDocument30 pagesAnti Diabetik A Oral: Dr. Theodorus, Mmedsc Staf Bagian Farmakologi FK UnsriDewi Putri Lenggo GeniNo ratings yet
- BiografieDocument73 pagesBiografieAna-Maria PantazicaNo ratings yet
- Microorganisms As BiofertilizerDocument16 pagesMicroorganisms As Biofertilizersivaram888No ratings yet
- Quiz On Prokaryotic DiversityDocument1 pageQuiz On Prokaryotic DiversityIbarra, Rachel B.No ratings yet
- Lab Report 1 SERIAL DILUTION OF MICROBIAL SAMPLEDocument6 pagesLab Report 1 SERIAL DILUTION OF MICROBIAL SAMPLERidma madusanka weerasinghaNo ratings yet
- G9 Science Q1 Week 3 4 Non Mendelian Patterns of InheritanDocument26 pagesG9 Science Q1 Week 3 4 Non Mendelian Patterns of InheritanSandra Lee LigsaNo ratings yet
- 2020 School of Medicine Textbooks MED1100, MED1200, MED2100, MED2200 Prescribed Author, Title, Edition PrescribedDocument4 pages2020 School of Medicine Textbooks MED1100, MED1200, MED2100, MED2200 Prescribed Author, Title, Edition PrescribedRobertNo ratings yet
- Imaging Protocol HandbookDocument90 pagesImaging Protocol HandbookAnita SzűcsNo ratings yet
- Resources 11 00015 v2Document20 pagesResources 11 00015 v2Gina M LópezNo ratings yet
- Ecosystem: BY: Jamaica R. AsuncionDocument21 pagesEcosystem: BY: Jamaica R. AsuncionJamaica AsuncionNo ratings yet
- 314 Biology SR Secondary Paper 2018Document11 pages314 Biology SR Secondary Paper 2018Vidya KoliNo ratings yet
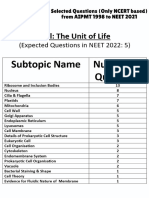
- Cell - The Unit of Life - NCERT Based PYQsDocument9 pagesCell - The Unit of Life - NCERT Based PYQsAkhil singhNo ratings yet
- RIZAL TECHNOLOGICAL UNIVERSITY Glossary of Key Environmental Engineering TermsDocument6 pagesRIZAL TECHNOLOGICAL UNIVERSITY Glossary of Key Environmental Engineering TermsMica GiananNo ratings yet
- Bio150-80 Syllabus-Instructor Addendum-2016 Fall PDFDocument5 pagesBio150-80 Syllabus-Instructor Addendum-2016 Fall PDFFatmata BanguraNo ratings yet
- Cell Poster ProjectDocument2 pagesCell Poster ProjectArita SabriuNo ratings yet
- BIOTECHNOLOGY SYLLABUS AND COURSE STRUCTUREDocument7 pagesBIOTECHNOLOGY SYLLABUS AND COURSE STRUCTURESheetal RajawatNo ratings yet
- Animal Kingdom Classification GuideDocument91 pagesAnimal Kingdom Classification GuideJoanna Susan JojiNo ratings yet
- First Grading Advance Science Reviewer Grade 7Document7 pagesFirst Grading Advance Science Reviewer Grade 7loraineNo ratings yet
- Prof. Yaron Ilan - Alimentary Pharmacology & TherapeuticsDocument15 pagesProf. Yaron Ilan - Alimentary Pharmacology & TherapeuticsProf. Yaron IlanNo ratings yet
- Read MeDocument3 pagesRead MeEubert OñezNo ratings yet
- SR5 TOOL Chrome Flesh IndexDocument2 pagesSR5 TOOL Chrome Flesh IndexBeki LokaNo ratings yet
- Animalia Part 1 Invertebrata PDFDocument46 pagesAnimalia Part 1 Invertebrata PDFTiara Safa EarleneNo ratings yet
- Placenta Extract & Castor Oil (Next Generation Wound Healer)Document11 pagesPlacenta Extract & Castor Oil (Next Generation Wound Healer)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Sequencing GuideDocument51 pagesSequencing GuideEmir SaricNo ratings yet