You might also like
- Breast Reviewer (2014)Document7 pagesBreast Reviewer (2014)Jade Monreal0% (1)
- Pathology 5.05b Vagina and Vulva - DR - Dy (Final Edit)Document11 pagesPathology 5.05b Vagina and Vulva - DR - Dy (Final Edit)Dranreb Berylle MasangkayNo ratings yet
- Pancreatic AdenocarcinomaDocument6 pagesPancreatic AdenocarcinomafikriafisNo ratings yet
- Case Presentation-ChickenpoxDocument41 pagesCase Presentation-ChickenpoxShaliniNo ratings yet
- Polycystic Kidney DiseaseDocument9 pagesPolycystic Kidney DiseaseCésar Aguilar ContrerasNo ratings yet
- Assessment of The Chest and Lungs: Pat Jackson AllenDocument50 pagesAssessment of The Chest and Lungs: Pat Jackson Allenbuzz Q100% (3)
- Acute Myeloid LeukemiaDocument45 pagesAcute Myeloid Leukemiasabila nugraha100% (1)
- Benign Gynecological LesionsDocument9 pagesBenign Gynecological LesionsLanceNo ratings yet
- Pathophysiology: Rectal CarcinomaDocument25 pagesPathophysiology: Rectal CarcinomaCristina CristinaNo ratings yet
- Essentials of Diagnosis and Treatment of Acute LeukemiaDocument16 pagesEssentials of Diagnosis and Treatment of Acute Leukemianouval_iqbalNo ratings yet
- #MediastinumDocument4 pages#Mediastinumameerabest100% (1)
- Abdominal MassDocument5 pagesAbdominal MassArthana PutraNo ratings yet
- Pathology Clinical Pathological CaseDocument4 pagesPathology Clinical Pathological CaseJulienne DelfinNo ratings yet
- Abdominal Trauma Signs, Symptoms and Nursing CareDocument24 pagesAbdominal Trauma Signs, Symptoms and Nursing CareSurgeryClassesNo ratings yet
- Gyne - Case 15 Benign Lesions of The Vulva & VaginaDocument2 pagesGyne - Case 15 Benign Lesions of The Vulva & Vaginacbac1990No ratings yet
- Benign & Precancerous Tumors of Female Genital Organs: by Assist. O.V.BakunDocument83 pagesBenign & Precancerous Tumors of Female Genital Organs: by Assist. O.V.BakunDian Permata PutraNo ratings yet
- Lower Gi Case Presentation PDFDocument35 pagesLower Gi Case Presentation PDFapi-448999672No ratings yet
- Cerebrospinal Fluid CSF Analysis and InterpretatioDocument6 pagesCerebrospinal Fluid CSF Analysis and InterpretatioIoana CucuNo ratings yet
- Vulvovaginal Candidiasis and Bacterial VaginosisDocument16 pagesVulvovaginal Candidiasis and Bacterial VaginosisAdnanda Maulan100% (1)
- 3 Year CPC October 8, 20202Document4 pages3 Year CPC October 8, 20202Raian SuyuNo ratings yet
- Phyllodes TumorDocument20 pagesPhyllodes TumorManuela KarinaaNo ratings yet
- ENDOCRINE PATHOLOGY WebpathDocument35 pagesENDOCRINE PATHOLOGY Webpathapi-3766657No ratings yet
- Hemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUDocument27 pagesHemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUAbdisalan hassanNo ratings yet
- Kaposis Sarcoma: Denis NahabweDocument32 pagesKaposis Sarcoma: Denis NahabwexilcomNo ratings yet
- Pathology B - Gastrointestinal Tract (Esguerra, 2015)Document18 pagesPathology B - Gastrointestinal Tract (Esguerra, 2015)Ars MoriendiNo ratings yet
- L6-PATHO-Neoplasia (Sept2821)Document12 pagesL6-PATHO-Neoplasia (Sept2821)Erald PaderangaNo ratings yet
- Medicine 6.1b Approach To Cancer Patients - FernandoDocument7 pagesMedicine 6.1b Approach To Cancer Patients - FernandoAbigail LausNo ratings yet
- 2017 Bethesda System of Reporting Thyroid CytopathologyDocument6 pages2017 Bethesda System of Reporting Thyroid CytopathologyLuisNo ratings yet
- Evaluation of Abdominal PainDocument7 pagesEvaluation of Abdominal PainCherry Faith Merisco LabtangNo ratings yet
- Inguinal Hernia EcaaDocument36 pagesInguinal Hernia EcaaElsha ZaskiaNo ratings yet
- Acute Post Streptococcal Glomerulonephritis: DiseaseDocument3 pagesAcute Post Streptococcal Glomerulonephritis: DiseaseHades Luciferos PallonesNo ratings yet
- Refkas CondylomaAccuminataDocument18 pagesRefkas CondylomaAccuminatamichelle1945No ratings yet
- Hypertension and Angina DrugsDocument158 pagesHypertension and Angina DrugsMelissa SalayogNo ratings yet
- Mucinous Cystadenoma 0708Document12 pagesMucinous Cystadenoma 0708eosfieldNo ratings yet
- Trans Congenital MalformationsDocument10 pagesTrans Congenital MalformationsRemelou Garchitorena AlfelorNo ratings yet
- Examination of Breast Lump PDFDocument2 pagesExamination of Breast Lump PDFDanaNo ratings yet
- 3 Surgery - Mediastinum and PleuraDocument6 pages3 Surgery - Mediastinum and PleuraCassey Koi FarmNo ratings yet
- Etiology of Cervical Cancer PDFDocument2 pagesEtiology of Cervical Cancer PDFBudNo ratings yet
- Bethesda system for reporting cervical cytologyDocument3 pagesBethesda system for reporting cervical cytologyNgotelo FunwiNo ratings yet
- Abdominal Examination Print PDFDocument8 pagesAbdominal Examination Print PDFPooja HbNo ratings yet
- Introduction To TransplantationDocument3 pagesIntroduction To TransplantationGerardLumNo ratings yet
- Opportunistic Mycoses: Yeasts: Candida SPP., Cryptococcus Spp. Mycelial or Filamentous FungiDocument10 pagesOpportunistic Mycoses: Yeasts: Candida SPP., Cryptococcus Spp. Mycelial or Filamentous FungiSSJ GAMERNo ratings yet
- Breast Pathology Fumc 2022Document145 pagesBreast Pathology Fumc 2022Bahzad AkramNo ratings yet
- MPNST Diagnosis and TreatmentDocument27 pagesMPNST Diagnosis and TreatmentrahadiyantiNo ratings yet
- Nematode Infections 2019 Student PDFDocument272 pagesNematode Infections 2019 Student PDFCharlene SuliganNo ratings yet
- RCJ Finals - Non Epithelial Ovarian CaDocument4 pagesRCJ Finals - Non Epithelial Ovarian CaJohn Paulo Catacutan100% (1)
- Differential Diagnosis of The Adnexal Mass 2020Document38 pagesDifferential Diagnosis of The Adnexal Mass 2020Sonia MVNo ratings yet
- Ovarian Tumor: Obstetrics & GynecologyDocument37 pagesOvarian Tumor: Obstetrics & GynecologyFathimathNo ratings yet
- Chronic Inflammation Guide: Causes, Types & PathogenesisDocument47 pagesChronic Inflammation Guide: Causes, Types & PathogenesisPradeepNo ratings yet
- Benign and Malignant Cervical LesionsDocument46 pagesBenign and Malignant Cervical LesionsRohitNo ratings yet
- Benign Cystic TeratomaDocument3 pagesBenign Cystic TeratomaLisa Dwipurnamasari TobingNo ratings yet
- Pathogens of The Female Reproductive System - Leah NechamkinDocument1 pagePathogens of The Female Reproductive System - Leah NechamkinMicroposterNo ratings yet
- Managing Nause and Vomiting-Crit-Care-Nurse-2003-Garrett-31-50 PDFDocument22 pagesManaging Nause and Vomiting-Crit-Care-Nurse-2003-Garrett-31-50 PDFpmuftiaNo ratings yet
- Case Study CA Lower RectumDocument47 pagesCase Study CA Lower RectumArtyom Granovskiy100% (1)
- Physical Examination of Urine: Analysis of Urine and Other Body Fluids Module 4Document19 pagesPhysical Examination of Urine: Analysis of Urine and Other Body Fluids Module 4Francis ValdezNo ratings yet
- DISC, Drugs, Infection, Thick Basal MembraneDocument5 pagesDISC, Drugs, Infection, Thick Basal MembraneHOPENo ratings yet
- Gallbladder and Pancrease PathologyDocument4 pagesGallbladder and Pancrease Pathologyjohn smithNo ratings yet
- Megaloblastic Anemias: Dept of Medicine AcmsDocument71 pagesMegaloblastic Anemias: Dept of Medicine Acmskunal ghosh100% (1)
- Stevens Johnson DiseaseDocument5 pagesStevens Johnson DiseaseShammy RNNo ratings yet
- Community-Acquired Pneumonia - CPG 2016Document26 pagesCommunity-Acquired Pneumonia - CPG 2016Jamie SebastianNo ratings yet
- SCREEM (Divina) resources pathology planDocument2 pagesSCREEM (Divina) resources pathology planDranreb Berylle MasangkayNo ratings yet
- Sexual Harassment Act FMCH April 2017Document29 pagesSexual Harassment Act FMCH April 2017Dranreb Berylle MasangkayNo ratings yet
- Sexually Transmitted Diseases de VeraDocument50 pagesSexually Transmitted Diseases de VeraDranreb Berylle MasangkayNo ratings yet
- CVS, Respi Heent ExamDocument8 pagesCVS, Respi Heent ExamDranreb Berylle MasangkayNo ratings yet
- Pathology 4.05 Liver Pathology - Dr. YanezDocument22 pagesPathology 4.05 Liver Pathology - Dr. YanezDranreb Berylle MasangkayNo ratings yet
- Pathology 4.05 Liver Pathology - Dr. YanezDocument22 pagesPathology 4.05 Liver Pathology - Dr. YanezDranreb Berylle MasangkayNo ratings yet
- C N L Part 1 - Diseases and Chest Pain TablesDocument3 pagesC N L Part 1 - Diseases and Chest Pain TablesDranreb Berylle MasangkayNo ratings yet
- C N L Part 1 - Diseases and Chest Pain TablesDocument3 pagesC N L Part 1 - Diseases and Chest Pain TablesDranreb Berylle MasangkayNo ratings yet
- Non-Pharmacological Treatment Lifestyle ModificationsDocument6 pagesNon-Pharmacological Treatment Lifestyle ModificationsDranreb Berylle MasangkayNo ratings yet
- What Is The Diagnosis? 2. Give The Basis For Your Diagnosis and Criteria For Your Diagnosis? SymptomsDocument1 pageWhat Is The Diagnosis? 2. Give The Basis For Your Diagnosis and Criteria For Your Diagnosis? SymptomsDranreb Berylle MasangkayNo ratings yet
- Family Structure, Characteristics and DynamicsDocument6 pagesFamily Structure, Characteristics and DynamicsErilyn Leigh ManaloNo ratings yet
- RepairDocument48 pagesRepairDranreb Berylle MasangkayNo ratings yet
- Stroke PDFDocument106 pagesStroke PDFDranreb Berylle MasangkayNo ratings yet
- Malabsorptive DiarrheaDocument3 pagesMalabsorptive DiarrheaDranreb Berylle MasangkayNo ratings yet
- EYE PATHOLOGIES REVEALEDDocument11 pagesEYE PATHOLOGIES REVEALEDDranreb Berylle MasangkayNo ratings yet
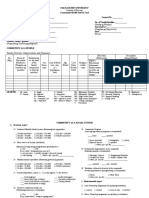
- Community Survey ToolDocument10 pagesCommunity Survey ToolDranreb Berylle MasangkayNo ratings yet
- Malabsorptive DiarrheaDocument3 pagesMalabsorptive DiarrheaDranreb Berylle MasangkayNo ratings yet
- Family Structure, Characteristics and DynamicsDocument6 pagesFamily Structure, Characteristics and DynamicsErilyn Leigh ManaloNo ratings yet
- CSTDocument36 pagesCSTDranreb Berylle MasangkayNo ratings yet
- Family Structure, Characteristics and DynamicsDocument6 pagesFamily Structure, Characteristics and DynamicsErilyn Leigh ManaloNo ratings yet
- CSTDocument36 pagesCSTDranreb Berylle MasangkayNo ratings yet
- 1malabsorption SyndromeDocument6 pages1malabsorption SyndromeDranreb Berylle MasangkayNo ratings yet
- CSTDocument36 pagesCSTDranreb Berylle MasangkayNo ratings yet
- Malabsorption: Exocrine Pancreatic InsufficiencyDocument6 pagesMalabsorption: Exocrine Pancreatic InsufficiencyDranreb Berylle MasangkayNo ratings yet
- Community Assessment Tools: A Companion Piece To Communities in ActionDocument12 pagesCommunity Assessment Tools: A Companion Piece To Communities in ActionDranreb Berylle MasangkayNo ratings yet
- Diarrhea (Autosaved)Document3 pagesDiarrhea (Autosaved)Dranreb Berylle MasangkayNo ratings yet
- Inflammatory Bowel DiseaseDocument19 pagesInflammatory Bowel DiseaseDranreb Berylle MasangkayNo ratings yet
- BioFluid Mechanics 1Document29 pagesBioFluid Mechanics 1roxannedemaeyerNo ratings yet
- Vitamins and Minerals Directly Involved in Energy MetabolismDocument5 pagesVitamins and Minerals Directly Involved in Energy MetabolismBaber Amin100% (1)
- Pioneers in Thyroid Surgery ARTICLEDocument12 pagesPioneers in Thyroid Surgery ARTICLESandu AlexandraNo ratings yet
- Disorders of Nutrition: Environmental PathologyDocument66 pagesDisorders of Nutrition: Environmental Pathologyjulo_05No ratings yet
- Alan Aragon Macro and Calorie Calculator Template 6Document8 pagesAlan Aragon Macro and Calorie Calculator Template 6tatiNo ratings yet
- Study of Biochemical Parameters in Nephrotic PatientsDocument57 pagesStudy of Biochemical Parameters in Nephrotic PatientsHimanshu MishraNo ratings yet
- Carotenoids and their role in nutritionDocument4 pagesCarotenoids and their role in nutritionSaravana KumarNo ratings yet
- Krok 1 Stomatology: Test Items For Licensing ExaminationDocument24 pagesKrok 1 Stomatology: Test Items For Licensing ExaminationhelloNo ratings yet
- Biopsy of Thyroid Gland: Diagnosing Thyroid ConditionsDocument5 pagesBiopsy of Thyroid Gland: Diagnosing Thyroid ConditionsPandesal with EggNo ratings yet
- Nutrition and Diet Therapy 6th Edition Lutz Test Bank DownloadDocument13 pagesNutrition and Diet Therapy 6th Edition Lutz Test Bank Downloadhanhcharmainee29v100% (26)
- Drug StudyDocument18 pagesDrug StudyAntonethe DemdamNo ratings yet
- Management of Hypothyroidism and Hypothyroxinemia During Pregnancy-AaceDocument8 pagesManagement of Hypothyroidism and Hypothyroxinemia During Pregnancy-Aacegu mailNo ratings yet
- Abbott Annual Report 2016Document80 pagesAbbott Annual Report 2016Ojo-publico.comNo ratings yet
- Netupitant 300mg + Palonosetron HCL 0.56mg (Akynzeo)Document16 pagesNetupitant 300mg + Palonosetron HCL 0.56mg (Akynzeo)ddandan_2No ratings yet
- Thiamine OriginalDocument10 pagesThiamine OriginalJehangir AllamNo ratings yet
- Brown Atrophy of the Heart Pathology Slide ExamDocument79 pagesBrown Atrophy of the Heart Pathology Slide ExamFYMNo ratings yet
- Clinical Chemistry 2Document65 pagesClinical Chemistry 2Jennifer BaluarteNo ratings yet
- ENT-Laryngeal ParalysisDocument26 pagesENT-Laryngeal ParalysisRahul Kumar DiwakarNo ratings yet
- Pain ManagementDocument32 pagesPain ManagementShania CandaNo ratings yet
- ABG Interpretation WorksheetDocument5 pagesABG Interpretation WorksheetArvee Caezar F. VizcarraNo ratings yet
- Ergogenic Aids That WorkDocument43 pagesErgogenic Aids That Workmahnoor fatimaNo ratings yet
- Hashimoto ThyroiditisDocument20 pagesHashimoto ThyroiditisMohd Akmal Nordin100% (1)
- Sytenol A Brochure Acne 2016Document8 pagesSytenol A Brochure Acne 2016dian kaizenNo ratings yet
- Aurora Poineeers Memeorial College Formerly: Cebuano Barracks Institute Aurora, Zamboanga Del Sur Final Examination College DepartmentDocument6 pagesAurora Poineeers Memeorial College Formerly: Cebuano Barracks Institute Aurora, Zamboanga Del Sur Final Examination College DepartmentEvaNo ratings yet
- University of Duhok College of Medicine Module of Metabolism Student Book 2021-2022Document213 pagesUniversity of Duhok College of Medicine Module of Metabolism Student Book 2021-2022QasmNo ratings yet
- Pancreas Neuroendocrine Tumors: An IntroductionDocument7 pagesPancreas Neuroendocrine Tumors: An IntroductionNoviari Liara JustitiaNo ratings yet
- LipoTrim Detail AidDocument15 pagesLipoTrim Detail AidDavid WeeNo ratings yet
- Neuromuscular Blocking DrugsDocument3 pagesNeuromuscular Blocking DrugsYogi drNo ratings yet
- Chemical Digestion and Absorption - A Closer Look - Anatomy and PhysiologyDocument20 pagesChemical Digestion and Absorption - A Closer Look - Anatomy and PhysiologyMa Mayla Imelda LapaNo ratings yet
- High Yield OSCE - SurgeryDocument2 pagesHigh Yield OSCE - SurgerymashupNo ratings yet