You might also like
- Ferron Glumin XRDocument22 pagesFerron Glumin XRhilmayuniarNo ratings yet
- STELLAR Study (Rosuvastatina)Document44 pagesSTELLAR Study (Rosuvastatina)ijido_sc100% (1)
- SAVOR TIMI 53 Presentation SlidesDocument29 pagesSAVOR TIMI 53 Presentation SlidesSheila ZivanaNo ratings yet
- ACARBOSE in The Treatment of T2DMDocument46 pagesACARBOSE in The Treatment of T2DMBudi WirawanNo ratings yet
- Formulary For Employe of Pharmacy PDFDocument59 pagesFormulary For Employe of Pharmacy PDFHanif khanNo ratings yet
- Chemo Stability Chart - LtoZDocument41 pagesChemo Stability Chart - LtoZOcy EmailNo ratings yet
- Spasm OmenDocument30 pagesSpasm OmenJehanzeb Tariq100% (1)
- UV-Raman method quality control anticancer preparationsDocument8 pagesUV-Raman method quality control anticancer preparationsAffrilinaNo ratings yet
- Naturex Gingest PDFDocument5 pagesNaturex Gingest PDFyuricpNo ratings yet
- Bemsivir: 210 X 148 MM 210 X 148 MMDocument2 pagesBemsivir: 210 X 148 MM 210 X 148 MMSaifur Rahman SuzonNo ratings yet
- EUROPEAN PHARMACOPOEIA 9.0 HUMAN NORMAL IMMUNOGLOBULINDocument3 pagesEUROPEAN PHARMACOPOEIA 9.0 HUMAN NORMAL IMMUNOGLOBULINdannny_mejiaaNo ratings yet
- NICE - Menopause Diagnosis and ManagementDocument30 pagesNICE - Menopause Diagnosis and Managementshrinkhala bhattaraiNo ratings yet
- Marketing Presentation 63Document16 pagesMarketing Presentation 63Soikot100% (1)
- Product Overview Product Overview: Difficile Associated DiarrheaDocument2 pagesProduct Overview Product Overview: Difficile Associated Diarrheamichael bundalianNo ratings yet
- Medication History Interview Form-MCP+OGH-PharmD VI Year InternshipDocument2 pagesMedication History Interview Form-MCP+OGH-PharmD VI Year InternshipMarifuddin HussainiNo ratings yet
- CPMP Code ensures rational medicine useDocument160 pagesCPMP Code ensures rational medicine useShimul HalderNo ratings yet
- Marketing Plan For XenicalDocument19 pagesMarketing Plan For XenicalAnonymous 75aETJ8O100% (1)
- AOE - Hiral Labs LTD Company Brochure 20180416170521Document20 pagesAOE - Hiral Labs LTD Company Brochure 20180416170521Dr VENKAT1 LUNo ratings yet
- AnxolamDocument38 pagesAnxolammanjitdeshmukh2No ratings yet
- Choosing The Right DPP-4i: Translating Evidence To PracticeDocument33 pagesChoosing The Right DPP-4i: Translating Evidence To PracticeRohit ThanageNo ratings yet
- Biogenix Catalogue enDocument84 pagesBiogenix Catalogue enMreis GestorNo ratings yet
- Ciplamed - Montair LC & Montair LC Kid DT - Syrup - 2018-03-20Document11 pagesCiplamed - Montair LC & Montair LC Kid DT - Syrup - 2018-03-20anon_458167643100% (1)
- Annual Report DHG Pharma 2014 - V1Document113 pagesAnnual Report DHG Pharma 2014 - V1Nguyễn Ánh100% (1)
- Chemo Stability Chart - AtoKDocument49 pagesChemo Stability Chart - AtoKDhafietBtSalimEl-NuruddinNo ratings yet
- APAP-McNeil Package-2002Document127 pagesAPAP-McNeil Package-2002qiuy99No ratings yet
- Mini RinDocument5 pagesMini Rinlovely_dyaNo ratings yet
- Aceclofenac Efficacy and Safety Vs DiclofenacDocument6 pagesAceclofenac Efficacy and Safety Vs DiclofenacpdelaxNo ratings yet
- Nursing Assessment ToolDocument6 pagesNursing Assessment ToolRaniNo ratings yet
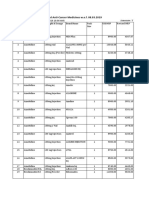
- Revised MRP of Non-Scheduled Anti-Cancer MedicinesDocument23 pagesRevised MRP of Non-Scheduled Anti-Cancer Medicinessampath seshadri100% (1)
- ChemoStabilityChart AtoK 14jan2014Document42 pagesChemoStabilityChart AtoK 14jan2014nofiasaridNo ratings yet
- Lista Me Cmimet e Barnave Jo Te Rimbursueshme 2014, 17feb2014Document340 pagesLista Me Cmimet e Barnave Jo Te Rimbursueshme 2014, 17feb2014Endri RamadaniNo ratings yet
- California 3 Tier Drug ListDocument156 pagesCalifornia 3 Tier Drug ListSangram KhandareNo ratings yet
- Global Albumin MarketDocument3 pagesGlobal Albumin MarketiHealthcareAnalyst, Inc.0% (1)
- Tramadol HydrochlorideDocument157 pagesTramadol HydrochlorideShahid LatifNo ratings yet
- 2152 Trifed 1444226440 PDFDocument1 page2152 Trifed 1444226440 PDFLouis WakumNo ratings yet
- Drug CompilationDocument39 pagesDrug CompilationANa AntonioNo ratings yet
- CataflyDocument16 pagesCataflyEbiyele Olusegun OwoturoNo ratings yet
- Drugs To Watch With WARFARINDocument3 pagesDrugs To Watch With WARFARINRajendra RaiNo ratings yet
- Nebesel LaunchPlDocument42 pagesNebesel LaunchPlPrithvi Raj100% (1)
- Updates On Metformin JDM2019 DTDocument37 pagesUpdates On Metformin JDM2019 DTLaurentius JohanNo ratings yet
- Humana Investor DayDocument100 pagesHumana Investor DaymedtechyNo ratings yet
- Ascorbic Acid Injection, USPDocument4 pagesAscorbic Acid Injection, USPYovie PrayektiNo ratings yet
- Liver Disease Diagnosis System Using Machine LearningDocument3 pagesLiver Disease Diagnosis System Using Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pharmacology Assignment - Medicines and MealsDocument15 pagesPharmacology Assignment - Medicines and MealsFarhat JahanNo ratings yet
- Safety Data Sheet Lubricool™ACDocument9 pagesSafety Data Sheet Lubricool™ACNur Cholis HadiNo ratings yet
- MSDS Bisoprolol Fumarate Tablets (Greenstone LLC) (EN)Document10 pagesMSDS Bisoprolol Fumarate Tablets (Greenstone LLC) (EN)ANNaNo ratings yet
- Ascoril Expectorant - FAQ'sDocument16 pagesAscoril Expectorant - FAQ'skurutalaNo ratings yet
- Formulation, Characterization of Pellets of Duloxetine Hydrochloride by Extrusion and SpheronizationDocument28 pagesFormulation, Characterization of Pellets of Duloxetine Hydrochloride by Extrusion and SpheronizationHely PatelNo ratings yet
- NeseritideDocument28 pagesNeseritideNavojit Chowdhury100% (1)
- EP1374874A2 Liquid Antacid CompositionsDocument6 pagesEP1374874A2 Liquid Antacid CompositionsKevin Alexander Campos De León100% (1)
- Jan AushadiDocument14 pagesJan AushadiJose PiusNo ratings yet
- Development of A Stable Oral Pediatric Solution of Hydrochlorothiazide by The Combined Use of Cyclodextrins and Hydrophilic PolymersDocument9 pagesDevelopment of A Stable Oral Pediatric Solution of Hydrochlorothiazide by The Combined Use of Cyclodextrins and Hydrophilic PolymersAntony Joel Meza LoardoNo ratings yet
- Essential Medicines Lists Punjab 2014Document65 pagesEssential Medicines Lists Punjab 2014Salman Nazir WattuNo ratings yet
- Tramadol OMSDocument39 pagesTramadol OMSFranco VairolettiNo ratings yet
- Hospira Plum A+ TSMDocument183 pagesHospira Plum A+ TSMbrianNo ratings yet
- Film-Coated Tablets for Bone HealthDocument1 pageFilm-Coated Tablets for Bone Healthpharmacist PUCPNo ratings yet
- Laporan Igd 2018Document216 pagesLaporan Igd 2018Rahma watiNo ratings yet
- 2014 Leaflet Dosage High-Resolution-1Document4 pages2014 Leaflet Dosage High-Resolution-1Zarbakht AliNo ratings yet
- Management: The Principles of Treatment of Chronic Pain in General Include The Following (WHO)Document19 pagesManagement: The Principles of Treatment of Chronic Pain in General Include The Following (WHO)ASMPH Pioneers DocumentsNo ratings yet
- Methocarbamol (Robaxin)Document1 pageMethocarbamol (Robaxin)ENo ratings yet
- Kertas Kerja PinjamanDocument18 pagesKertas Kerja PinjamanWan AzmanNo ratings yet
- Unveiling Tetanus A Comprehensive Exploration of The Causes Symptoms Prevention and TreatmentDocument12 pagesUnveiling Tetanus A Comprehensive Exploration of The Causes Symptoms Prevention and TreatmentMikhil mchaeladdictionsNo ratings yet
- Gastrointestinal Parasites of ElephantDocument8 pagesGastrointestinal Parasites of ElephantDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU Philippines100% (2)
- Full Download High Acuity Nursing 6th Edition Wagner Test BankDocument18 pagesFull Download High Acuity Nursing 6th Edition Wagner Test Bankassapancopepodmhup100% (38)
- 3911515Document1 page3911515Gemmelle CangcoNo ratings yet
- Nutrients: Protein Nutrition and Malnutrition in CKD and ESRDDocument19 pagesNutrients: Protein Nutrition and Malnutrition in CKD and ESRDrandy_27995No ratings yet
- Alemitu MequanintDocument125 pagesAlemitu MequanintshegawNo ratings yet
- Prak Ospe PK FMS 3 2021Document7 pagesPrak Ospe PK FMS 3 2021Angelique NatalieNo ratings yet
- Clinical Manifestations and Management of Hospitalized Women With Bartholin Versus Non Bartholin Vulvar AbscessDocument4 pagesClinical Manifestations and Management of Hospitalized Women With Bartholin Versus Non Bartholin Vulvar AbscessPaul HartingNo ratings yet
- Standard LFT and It's Clinical SignificanceDocument28 pagesStandard LFT and It's Clinical SignificanceanimathzNo ratings yet
- Chapter Eight 8.0 Environmental Management and Safety 8.1 General IntroductionDocument8 pagesChapter Eight 8.0 Environmental Management and Safety 8.1 General IntroductionRichard ObinnaNo ratings yet
- AOAC Rapid Method ValidationDocument60 pagesAOAC Rapid Method ValidationPiruzi MaghlakelidzeNo ratings yet
- Blueprint of LifeDocument11 pagesBlueprint of Lifetimeflies23No ratings yet
- DNA RepairDocument35 pagesDNA RepairAbid Al RezaNo ratings yet
- What Is Hiv/Aids?: Human Immunodeficiency Virus (Hiv)Document2 pagesWhat Is Hiv/Aids?: Human Immunodeficiency Virus (Hiv)Rockie Geronda EsmaneNo ratings yet
- Hand Hygiene Self Assessment FrameworkDocument9 pagesHand Hygiene Self Assessment FrameworkWiDya EmiLiaNo ratings yet
- Pol TakesDocument84 pagesPol Takesfauzi jayaNo ratings yet
- 2562 - PDF OmigatDocument11 pages2562 - PDF OmigatkhansarafidaNo ratings yet
- PharmacokineticsDocument7 pagesPharmacokineticsRonica MendozaNo ratings yet
- 7 Vs 14days Gram Negative SepsisDocument8 pages7 Vs 14days Gram Negative SepsisPavan KumarNo ratings yet
- Cardiovascular System AgingDocument17 pagesCardiovascular System Agingapi-541796556No ratings yet
- 3rdQ Health DLLDocument4 pages3rdQ Health DLLMichelle Handumon Alviar85% (13)
- Introduction PRDS and APRDSDocument13 pagesIntroduction PRDS and APRDSPrudhvi RajNo ratings yet
- Leafy Vegetables HarvestingDocument18 pagesLeafy Vegetables HarvestingSonia BadaNo ratings yet
- Paediatric Examination Handbook 2015Document66 pagesPaediatric Examination Handbook 2015Ulfa Rahmadanti SetiawanNo ratings yet
- Internal Medicine 5th MidtermDocument13 pagesInternal Medicine 5th MidtermIashdip iashdipNo ratings yet
- Chorti DictionaryDocument285 pagesChorti DictionaryLuis Bedoya100% (1)
- Manual of TB and Leprosy in TanzaniaDocument132 pagesManual of TB and Leprosy in TanzaniaYovanRivanzahNo ratings yet
- CogwheelDocument4 pagesCogwheelRimsha RanaNo ratings yet
- Hot and Cold Application - PPTX RevisedDocument61 pagesHot and Cold Application - PPTX RevisedMicah HuanNo ratings yet