You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Jurding RadioDocument11 pagesJurding RadioMutiara Sri WidyastutiNo ratings yet
- Management of Hyperglycemia in Diabetes MellitusDocument8 pagesManagement of Hyperglycemia in Diabetes MellitusMutiara Sri WidyastutiNo ratings yet
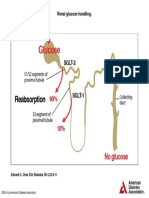
- Renal Glucose Handling.: Edward C. Chao Clin Diabetes 2014 32:4-11Document1 pageRenal Glucose Handling.: Edward C. Chao Clin Diabetes 2014 32:4-11Mutiara Sri WidyastutiNo ratings yet
- SGLT-2 Mediates Glucose Reabsorption in The Kidney.: Edward C. Chao Clin Diabetes 2014 32:4-11Document1 pageSGLT-2 Mediates Glucose Reabsorption in The Kidney.: Edward C. Chao Clin Diabetes 2014 32:4-11Mutiara Sri WidyastutiNo ratings yet
- Lecture Notes ENTDocument190 pagesLecture Notes ENTKamar Fletcher100% (3)
- 4Document8 pages4Mutiara Sri WidyastutiNo ratings yet
- Renal glucose handling before and after SGLT-2 inhibitionDocument1 pageRenal glucose handling before and after SGLT-2 inhibitionMutiara Sri WidyastutiNo ratings yet
- Diagnosis and Management of Bronchial AsthmaDocument8 pagesDiagnosis and Management of Bronchial AsthmaNidiah100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Laser Surface Treatment ProcessesDocument63 pagesLaser Surface Treatment ProcessesDIPAK VINAYAK SHIRBHATENo ratings yet
- Ultrasonic Weld Examination ProcedureDocument16 pagesUltrasonic Weld Examination ProcedureramalingamNo ratings yet
- SECTION 303-06 Starting SystemDocument8 pagesSECTION 303-06 Starting SystemTuan TranNo ratings yet
- ASA 2018 Catalog WebDocument48 pagesASA 2018 Catalog WebglmedinaNo ratings yet
- Space DynamicsDocument37 pagesSpace Dynamicspurushottam KashyapNo ratings yet
- Innovative Food Science and Emerging TechnologiesDocument6 pagesInnovative Food Science and Emerging TechnologiesAnyelo MurilloNo ratings yet
- Survey Report on Status of Chemical and Microbiological Laboratories in NepalDocument38 pagesSurvey Report on Status of Chemical and Microbiological Laboratories in NepalGautam0% (1)
- Cost Analysis and Financial Projections for Gerbera Cultivation ProjectDocument26 pagesCost Analysis and Financial Projections for Gerbera Cultivation ProjectshroffhardikNo ratings yet
- Guidance Notes Blow Out PreventerDocument6 pagesGuidance Notes Blow Out PreventerasadqhseNo ratings yet
- Madeleine Ker - TakeoverDocument91 pagesMadeleine Ker - Takeover66677785100% (1)
- Activities and Assessments:: ASSIGNMENT (SUBMIT Your Answers at EDMODO Assignment Section)Document5 pagesActivities and Assessments:: ASSIGNMENT (SUBMIT Your Answers at EDMODO Assignment Section)Quen CuestaNo ratings yet
- 中美两国药典药品分析方法和方法验证Document72 pages中美两国药典药品分析方法和方法验证JasonNo ratings yet
- Flexibility Personal ProjectDocument34 pagesFlexibility Personal Projectapi-267428952100% (1)
- Clean Milk ProductionDocument19 pagesClean Milk ProductionMohammad Ashraf Paul100% (3)
- (Razavi) Design of Analog Cmos Integrated CircuitsDocument21 pages(Razavi) Design of Analog Cmos Integrated CircuitsNiveditha Nivi100% (1)
- Internship ReportDocument18 pagesInternship ReportRathan Kumar SMNo ratings yet
- Gas Natural Aplicacion Industria y OtrosDocument319 pagesGas Natural Aplicacion Industria y OtrosLuis Eduardo LuceroNo ratings yet
- 2019 Course CatalogDocument31 pages2019 Course CatalogDeepen SharmaNo ratings yet
- Rectifiers and FiltersDocument68 pagesRectifiers and FiltersMeheli HalderNo ratings yet
- DR-M260 User Manual ENDocument87 pagesDR-M260 User Manual ENMasa NourNo ratings yet
- Emerson EPC48150 1800 FA1EPC48300 3200 FA1 V PDFDocument26 pagesEmerson EPC48150 1800 FA1EPC48300 3200 FA1 V PDFRicardo Andrés Soto Salinas RassNo ratings yet
- SRS Design Guidelines PDFDocument46 pagesSRS Design Guidelines PDFLia FernandaNo ratings yet
- Life of A Landfill PumpDocument50 pagesLife of A Landfill PumpumidNo ratings yet
- Juan Martin Garcia System Dynamics ExercisesDocument294 pagesJuan Martin Garcia System Dynamics ExercisesxumucleNo ratings yet
- Liquid Out, Temperature 25.5 °C Tube: M/gs P / WDocument7 pagesLiquid Out, Temperature 25.5 °C Tube: M/gs P / WGianra RadityaNo ratings yet
- Digital Communication QuestionsDocument14 pagesDigital Communication QuestionsNilanjan BhattacharjeeNo ratings yet
- India - Wikipedia, The Free EncyclopediaDocument40 pagesIndia - Wikipedia, The Free EncyclopediaPrashanth KrishNo ratings yet
- Evolutionary PsychologyDocument10 pagesEvolutionary PsychologyShreya MadheswaranNo ratings yet
- CP 343-1Document23 pagesCP 343-1Yahya AdamNo ratings yet
- Pitch Manual SpecializedDocument20 pagesPitch Manual SpecializedRoberto Gomez100% (1)