You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Gallucci (2004) - Immediate Loading With Fixed Screw-Retained Provisional Restorations in Edentulous Jaws, The Pickup Technique.Document10 pagesGallucci (2004) - Immediate Loading With Fixed Screw-Retained Provisional Restorations in Edentulous Jaws, The Pickup Technique.Antonio González RuizNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- 2006 - Zuchelli - Predetermine The Line of Root Coverage PDFDocument8 pages2006 - Zuchelli - Predetermine The Line of Root Coverage PDFAntonio González RuizNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Zygomatic ImplantDocument18 pagesZygomatic ImplantsmritinarayanNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- 2006 - Zuchelli - Predetermine The Line of Root Coverage PDFDocument8 pages2006 - Zuchelli - Predetermine The Line of Root Coverage PDFAntonio González RuizNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Osteoporosis Diagnosis & Management: DR Aditya Kundu JR1 Department of Orthopedics, CNMC&HDocument53 pagesOsteoporosis Diagnosis & Management: DR Aditya Kundu JR1 Department of Orthopedics, CNMC&HAditya KunduNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Host Modulation Therapy - An Innovative Paradigm inDocument8 pagesHost Modulation Therapy - An Innovative Paradigm inpaper kitaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Mechanisms and Treatment of Hypercalcemia of MalignancyDocument8 pagesMechanisms and Treatment of Hypercalcemia of MalignancyDebby Christiana SNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 2003, Vol.32, Issues 2, Consultative EndocrinologyDocument210 pages2003, Vol.32, Issues 2, Consultative Endocrinologyomar ramirezNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
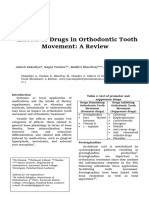
- Effects of Drugs in Orthodontic Tooth Movement: A ReviewDocument6 pagesEffects of Drugs in Orthodontic Tooth Movement: A ReviewvprakshaindiaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Anil S Et Al 2013 (Impact of Osteoporosis)Document7 pagesAnil S Et Al 2013 (Impact of Osteoporosis)Silviani FatmaNo ratings yet
- CDK Edisi CME-2 TH 2020 5 SKP PDFDocument24 pagesCDK Edisi CME-2 TH 2020 5 SKP PDFnarinaaviNo ratings yet
- Bisphosphonate and Dental Implant (Power Point) (FINAL)Document30 pagesBisphosphonate and Dental Implant (Power Point) (FINAL)Shehab RehanyNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Review Article Review Article Review ArticleDocument3 pagesReview Article Review Article Review ArticleNada SavitriNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Editorial: Dental Caries and OsteoporosisDocument2 pagesEditorial: Dental Caries and OsteoporosisBagis Emre GulNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- INBDEBooster Oral Medicine NotesDocument52 pagesINBDEBooster Oral Medicine NotesHelena Kalmat100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- 2021 ReviewDocument31 pages2021 ReviewRhum ImalinaNo ratings yet
- Biology 310 Assignment OsteoporosisDocument24 pagesBiology 310 Assignment OsteoporosisMohd IzwanNo ratings yet
- Effect of Intravenous Pamidronate Treatment in Children With Osteogenesis ImperfectaDocument5 pagesEffect of Intravenous Pamidronate Treatment in Children With Osteogenesis Imperfectavikash singhNo ratings yet
- Musculoskeletal DisordersDocument158 pagesMusculoskeletal DisordersJona Kristin EnclunaNo ratings yet
- Adams4e Tif Ch47Document19 pagesAdams4e Tif Ch47fbernis1480_11022046100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 70 MG Once Weekly For Mrs. CordovaDocument2 pages70 MG Once Weekly For Mrs. CordovaSherrie Ann Delos SantosNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Use of Bisphosphonates in Children. Review of The Literature and Guidelines For Dental ManagementDocument11 pagesThe Use of Bisphosphonates in Children. Review of The Literature and Guidelines For Dental ManagementHemil Dario Rosales MolinaNo ratings yet
- A Review On The Diseases and Treatments That Affect The Bone Physiology and StrengthDocument17 pagesA Review On The Diseases and Treatments That Affect The Bone Physiology and StrengthErnest Gabriel Cruz AdvinculaNo ratings yet
- Prevention - August 2016 USADocument100 pagesPrevention - August 2016 USATanya Hernandez100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- UTI FemaleDocument71 pagesUTI FemaledrsadafrafiNo ratings yet
- Pharmacokinetics of AlendronateDocument14 pagesPharmacokinetics of AlendronateSalsaNo ratings yet
- Drugs Med-SurgTest 3Document6 pagesDrugs Med-SurgTest 3Sarah PlunkettNo ratings yet
- Case Study About: OsteoporosisDocument15 pagesCase Study About: OsteoporosisAlliana Denice VicencioNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Drug Classifications for Arthritis & GoutDocument3 pagesDrug Classifications for Arthritis & GoutCindy100% (1)
- AAP Perio Lit Rev 1996-2010 - ImplantsDocument36 pagesAAP Perio Lit Rev 1996-2010 - ImplantsZhiyi LinNo ratings yet
- Human Anatomy and Physiology: Functions of the Skeletal and Muscular SystemsDocument43 pagesHuman Anatomy and Physiology: Functions of the Skeletal and Muscular SystemsJezebel MolinoNo ratings yet
- Guia Manejo Osteoporosis 2019Document28 pagesGuia Manejo Osteoporosis 2019SMIBA MedicinaNo ratings yet
- Osteoporosis y COVID19 InglesDocument5 pagesOsteoporosis y COVID19 Inglescesar kevin lopez marquezNo ratings yet
- Foxamax and Iboprofen Drug StudyDocument4 pagesFoxamax and Iboprofen Drug Studyaaron tabernaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)