You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- High performance BodyWave tanning and beauty machineDocument11 pagesHigh performance BodyWave tanning and beauty machinetranspotNo ratings yet
- Pulmonary Edema: Nuala J. Meyer,, - Michael A. MatthayDocument33 pagesPulmonary Edema: Nuala J. Meyer,, - Michael A. MatthayRaul JimenezNo ratings yet
- Physiology of MicrocirculationDocument93 pagesPhysiology of MicrocirculationMuskan RastogiNo ratings yet
- Sepsis and The Microcirculation: The Impact On Outcomes: ReviewDocument6 pagesSepsis and The Microcirculation: The Impact On Outcomes: ReviewDayanara DíazNo ratings yet
- 9-in-1 Beauty Machine User ManualDocument81 pages9-in-1 Beauty Machine User ManualMoises ReznikNo ratings yet
- Pathogenesis of Periodontal Disease د.فراسDocument11 pagesPathogenesis of Periodontal Disease د.فراسmayssam adnanNo ratings yet
- Gelofusine®: Stop Infusion andDocument2 pagesGelofusine®: Stop Infusion andRudy Arindra WijayaNo ratings yet
- Type2 DiabetesITO13jn PDFDocument543 pagesType2 DiabetesITO13jn PDFVanroNo ratings yet
- Inflammation GuideDocument70 pagesInflammation GuidemikeNo ratings yet
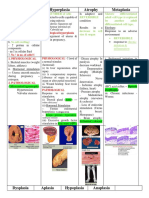
- Hypertrophy Hyperplasia Atrophy MetaplasiaDocument20 pagesHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNo ratings yet
- Clinical Case Study Guide - Cardiopulmonary Physical Therapy 3ed PDFDocument245 pagesClinical Case Study Guide - Cardiopulmonary Physical Therapy 3ed PDFraquelbibi0% (1)
- Anatomy and Pa Tho Physiology of Aqueous Production and OutflowDocument34 pagesAnatomy and Pa Tho Physiology of Aqueous Production and OutflowChristine TanNo ratings yet
- Cardiovascular Physiology - Achilles Pappano, 10EDocument305 pagesCardiovascular Physiology - Achilles Pappano, 10EPanda Mimi100% (1)
- Scalloped Tongue - Treatment Symptoms and Causes - Scalloped TongueDocument7 pagesScalloped Tongue - Treatment Symptoms and Causes - Scalloped TongueJing CruzNo ratings yet
- Pathophysiology of Cardiogenic Pulmonary EdemaDocument13 pagesPathophysiology of Cardiogenic Pulmonary EdemaIrina DuceacNo ratings yet
- Acute Pulmonary OdemaDocument9 pagesAcute Pulmonary OdemaAnonymous ysrxggk21cNo ratings yet
- Starling ForcesDocument2 pagesStarling ForcesMerlyn Chrislia RumtheNo ratings yet
- 2020 MONITORING COHERENCE Hemodynamic Coherence and The Rationale For MONITORING PDFDocument13 pages2020 MONITORING COHERENCE Hemodynamic Coherence and The Rationale For MONITORING PDFLUIS CARLOS MAYANo ratings yet
- Human Anat 2 Year Volume 4Document122 pagesHuman Anat 2 Year Volume 4HARSHINI PANDIANNo ratings yet
- Nobivac Piro Epar Scientific Discussion - en PDFDocument21 pagesNobivac Piro Epar Scientific Discussion - en PDFkuldeep sainiNo ratings yet
- Arterial HyperemyDocument10 pagesArterial HyperemyRohit NaiduNo ratings yet
- Renal MicrocirculationDocument33 pagesRenal MicrocirculationwiamNo ratings yet
- Magnet Space Materijal ENGDocument40 pagesMagnet Space Materijal ENGIvana MilosavljevicNo ratings yet
- J Survophthal 2018 10 005Document28 pagesJ Survophthal 2018 10 005Luis LondoñoNo ratings yet
- 1.traditional Chinese Medicine CuppingDocument5 pages1.traditional Chinese Medicine Cuppingnashrullah JamaluddinNo ratings yet
- Perio Lec.9 Pathogenesis o Periodontal DiseasesDocument32 pagesPerio Lec.9 Pathogenesis o Periodontal DiseasesزينNo ratings yet
- Complications of Injectable Fillers, Part 2: Vascular ComplicationsDocument17 pagesComplications of Injectable Fillers, Part 2: Vascular ComplicationsIsabel JiménezNo ratings yet
- Sean Walsh, Emma King - Pulse Diagnosis - A Clinical Guide, 1e-Churchill Livingstone (2007) PDFDocument427 pagesSean Walsh, Emma King - Pulse Diagnosis - A Clinical Guide, 1e-Churchill Livingstone (2007) PDFLM_S_S100% (1)
- Selected Readings in Plastic SurgeryDocument65 pagesSelected Readings in Plastic Surgeryleozee100% (6)