You might also like
- Final Assessing Female and Male Genitourinary SystemDocument7 pagesFinal Assessing Female and Male Genitourinary SystemJo Marchianne PigarNo ratings yet
- Case Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyDocument46 pagesCase Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyAjiMary M. DomingoNo ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- HemorrhoidsDocument26 pagesHemorrhoidsDini Norviatin0% (1)
- Lecture Contents: Definitions Composition of Hernia Managment of HerniaDocument26 pagesLecture Contents: Definitions Composition of Hernia Managment of Herniaissam_1994No ratings yet
- Why Is The Penis Shaped Like That? and Other Reflections On Being HumanDocument11 pagesWhy Is The Penis Shaped Like That? and Other Reflections On Being HumanMacmillan Publishers0% (1)
- Hypospadia and UTI CareDocument116 pagesHypospadia and UTI CareRhona ObiceNo ratings yet
- Testicular Tumor - Dr. FaizDocument54 pagesTesticular Tumor - Dr. FaizFemale calmNo ratings yet
- Sudden Sensorineural Hearing LossDocument26 pagesSudden Sensorineural Hearing LossSarah Nadia RasidiNo ratings yet
- Undescended Testis: DR - Santosh Jha TMUDocument33 pagesUndescended Testis: DR - Santosh Jha TMUYamir Fernando Monroy MartínNo ratings yet
- Internal Medicine Case Write Up 1Document14 pagesInternal Medicine Case Write Up 1Roshandiep GillNo ratings yet
- Operative Procedures: 1130 SRB's Manual of SurgeryDocument1 pageOperative Procedures: 1130 SRB's Manual of SurgerymadhuNo ratings yet
- AppendectomyDocument37 pagesAppendectomyRaquid MariaNo ratings yet
- Head Injury 5Document68 pagesHead Injury 5drvishal bhattNo ratings yet
- Intestinal Obstruction: Methas Arunnart MDDocument42 pagesIntestinal Obstruction: Methas Arunnart MDJhe-sie AngelinaNo ratings yet
- ThyroidectomyDocument17 pagesThyroidectomyDaryl Joshua SaturnoNo ratings yet
- Complication of Peptic Ulcer: Department of Surgery S. S. Medical College Rewa and Associate GMH and SGMH RewaDocument76 pagesComplication of Peptic Ulcer: Department of Surgery S. S. Medical College Rewa and Associate GMH and SGMH RewaBrajesh MouryaNo ratings yet
- Nursing Care of A Family C NewbornDocument18 pagesNursing Care of A Family C NewbornAudreySalvadorNo ratings yet
- Liver Abscess Clinical Presentation - History, Physical Examination, ComplicationsDocument2 pagesLiver Abscess Clinical Presentation - History, Physical Examination, ComplicationsAdi Kurnia100% (1)
- Testicular TorsionDocument20 pagesTesticular TorsionGAURAV100% (3)
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Blood TransfusionDocument14 pagesBlood TransfusionSarah Uy CaronanNo ratings yet
- Principles of Neonatal SurgeryDocument44 pagesPrinciples of Neonatal Surgerykbmed2003100% (2)
- 02 Skills LabDocument28 pages02 Skills Labivy annNo ratings yet
- 1.40 (Surgery) GIT Surgical Diseases - Diagnostics - Obesity ManagementDocument10 pages1.40 (Surgery) GIT Surgical Diseases - Diagnostics - Obesity ManagementLeo Mari Go LimNo ratings yet
- Case Presentation on Urethral StrictureDocument43 pagesCase Presentation on Urethral StrictureNadila Ayu Putri50% (2)
- Anaesthesia in Emergency Laparotomy: Speaker:P.Shravani Moderator:Dr.K.Vinay Assistant ProfessorDocument52 pagesAnaesthesia in Emergency Laparotomy: Speaker:P.Shravani Moderator:Dr.K.Vinay Assistant ProfessorSanthi Swetha PudhotaNo ratings yet
- HTN EmergencyDocument11 pagesHTN EmergencyKaran ChhabraNo ratings yet
- HyphemaDocument19 pagesHyphemaLiyanti RinceNo ratings yet
- Non-Variceal Upper GI Bleeding GuideDocument34 pagesNon-Variceal Upper GI Bleeding GuideChe Ainil ZainodinNo ratings yet
- St. Paul University Quezon City College of Health Sciences case study on CholedocholithiasisDocument5 pagesSt. Paul University Quezon City College of Health Sciences case study on CholedocholithiasisJanelle Kate SaleNo ratings yet
- Difficulty in Speech After StrokeDocument6 pagesDifficulty in Speech After StrokeAJ RegaladoNo ratings yet
- Kawasaki Disease DiagnosisDocument5 pagesKawasaki Disease DiagnosisFranz SalazarNo ratings yet
- Pre-Op Case Protocol #4Document2 pagesPre-Op Case Protocol #4IC BNo ratings yet
- Case Presentation On Supraventricular TachycardiaDocument64 pagesCase Presentation On Supraventricular TachycardiaHazel AsperaNo ratings yet
- The Hydrocephalus Foundation of The Philippines, Inc.: Save A Life, I PledgeDocument4 pagesThe Hydrocephalus Foundation of The Philippines, Inc.: Save A Life, I PledgejomitraNo ratings yet
- Hypospadias: by Khaled Ashour John Radcliffe HsopitalDocument87 pagesHypospadias: by Khaled Ashour John Radcliffe Hsopitalhayssam rashwanNo ratings yet
- Causes and Symptoms of Nontoxic GoiterDocument17 pagesCauses and Symptoms of Nontoxic Goiterabigaille chua100% (1)
- Systemic Surgery NuggetsDocument17 pagesSystemic Surgery NuggetsAhmad UsmanNo ratings yet
- UTI - Internship PresentationDocument27 pagesUTI - Internship PresentationPernel Jose Alam MicuboNo ratings yet
- Muscle Relaxants Classification and Mechanisms of ActionDocument22 pagesMuscle Relaxants Classification and Mechanisms of Actionvinay0717100% (1)
- Post Test Upper Gi BleedingDocument4 pagesPost Test Upper Gi BleedingMardie ArcesNo ratings yet
- IntussusceptionDocument33 pagesIntussusceptionNovendi RizkaNo ratings yet
- Cryptorchidism: The Absence of One or Both Testes From The ScrotumDocument7 pagesCryptorchidism: The Absence of One or Both Testes From The ScrotumClaudetteanne6171No ratings yet
- Inguinal HerniaDocument19 pagesInguinal HerniaAyu W. AnggreniNo ratings yet
- Surgery Case AppendicitisDocument30 pagesSurgery Case AppendicitisSarahNo ratings yet
- Massive Ventral Hernia Case StudyDocument7 pagesMassive Ventral Hernia Case StudysugisweNo ratings yet
- Case ReportDocument19 pagesCase ReportvivitaslimNo ratings yet
- Meniere's Disease.Document30 pagesMeniere's Disease.June Yasa HacheroNo ratings yet
- General Management of PoisoningDocument22 pagesGeneral Management of Poisoningranjithajay100% (1)
- Tibial FractureDocument6 pagesTibial FractureKristene June Ilagan CoyamNo ratings yet
- Fractured Femur Nursing CareDocument26 pagesFractured Femur Nursing CareMizzNina NyLeaNo ratings yet
- Introduction of Pediatric Nursing: Om Nursing Academy Anil Kantiwal Gudha (Whatsapp 9694936335)Document4 pagesIntroduction of Pediatric Nursing: Om Nursing Academy Anil Kantiwal Gudha (Whatsapp 9694936335)Preeti ChouhanNo ratings yet
- SurgeryDocument12 pagesSurgeryManusheeNo ratings yet
- Case Presentation Meyke Liechandra C11109130 Fracture ClavicleDocument24 pagesCase Presentation Meyke Liechandra C11109130 Fracture ClavicleWahyunita IlhamNo ratings yet
- IV Injection Evaluation ChecklistDocument2 pagesIV Injection Evaluation Checklistmaria hmNo ratings yet
- HEMEPARESISDocument18 pagesHEMEPARESISHari EshwaranNo ratings yet
- Case Presentation IM DDHDocument12 pagesCase Presentation IM DDHAishwarya BharathNo ratings yet
- Chronic Suppurative Otitis MediaDocument6 pagesChronic Suppurative Otitis MediaSuhas IngaleNo ratings yet
- Mitral Stenosis, NicvdDocument33 pagesMitral Stenosis, NicvdNavojit ChowdhuryNo ratings yet
- Liver Disease in 30-Year-Old FarmerDocument5 pagesLiver Disease in 30-Year-Old FarmerKanwaljeet SinghNo ratings yet
- 21 - Postoperative Complications and Managament IDocument30 pages21 - Postoperative Complications and Managament IAmmarNo ratings yet
- Notes On History Taking in The Cardiovascular SystemDocument10 pagesNotes On History Taking in The Cardiovascular Systemmdjohar72No ratings yet
- Amenorrhea: Definition - This Is The Symptom of Absence of MenstruationDocument10 pagesAmenorrhea: Definition - This Is The Symptom of Absence of MenstruationSuhas IngaleNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Anechoic Renal Masses: Differential Diagnosis and Imaging FindingsDocument9 pagesAnechoic Renal Masses: Differential Diagnosis and Imaging FindingsalaaNo ratings yet
- Acute Scrotal Swelling & Pain in ChildrenDocument58 pagesAcute Scrotal Swelling & Pain in ChildrenalaaNo ratings yet
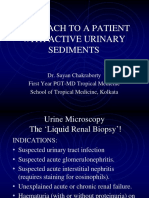
- Approach To A Patient With Active Urinary SedimentsDocument73 pagesApproach To A Patient With Active Urinary SedimentsalaaNo ratings yet
- American ImpotenceDocument259 pagesAmerican ImpotencealaaNo ratings yet
- Anechoic Renal Masses: Differential Diagnosis and Imaging FindingsDocument9 pagesAnechoic Renal Masses: Differential Diagnosis and Imaging FindingsalaaNo ratings yet
- Post Sleeve DeitDocument8 pagesPost Sleeve DeitalaaNo ratings yet
- Weight LossDocument10 pagesWeight LossalaaNo ratings yet
- GERD and Obesity: Impact of Sleeve GastrectomyDocument6 pagesGERD and Obesity: Impact of Sleeve GastrectomyalaaNo ratings yet
- Surgery in Morbid ObesityDocument28 pagesSurgery in Morbid ObesityalaaNo ratings yet
- Sleeve 3Document6 pagesSleeve 3alaaNo ratings yet
- Magenstrasse GastroplastyDocument8 pagesMagenstrasse GastroplastyalaaNo ratings yet
- Diagnosis and Classification of Urethral InjuriesDocument13 pagesDiagnosis and Classification of Urethral Injuriesleo100% (2)
- Sleeve LeakageDocument9 pagesSleeve LeakagealaaNo ratings yet
- Sleeve ComplicationsDocument6 pagesSleeve ComplicationsalaaNo ratings yet
- Sleeve 2Document22 pagesSleeve 2alaaNo ratings yet
- Sleeve Gastrectomy 1Document3 pagesSleeve Gastrectomy 1alaaNo ratings yet
- Surgical TTT of Penile Fracture PDFDocument2 pagesSurgical TTT of Penile Fracture PDFalaaNo ratings yet
- Xanthogranulomatous PyelonephritisDocument14 pagesXanthogranulomatous PyelonephritisalaaNo ratings yet
- Penile Fracture Not So RareDocument3 pagesPenile Fracture Not So RarealaaNo ratings yet
- Traumatic Rupture of Corpus CavernosumDocument6 pagesTraumatic Rupture of Corpus CavernosumalaaNo ratings yet
- Penoscrotal DeglovingDocument6 pagesPenoscrotal DeglovingalaaNo ratings yet
- Delayed Consultation and Treatment of Penile FractureDocument2 pagesDelayed Consultation and Treatment of Penile FracturealaaNo ratings yet
- Penile Fracure Causes & TTTDocument4 pagesPenile Fracure Causes & TTTalaaNo ratings yet
- Clinical Diagnosis of Penile FractureDocument3 pagesClinical Diagnosis of Penile FracturealaaNo ratings yet
- False Fracture of The PenisDocument4 pagesFalse Fracture of The PenisalaaNo ratings yet
- Diagnosis and Classification of Urethral InjuriesDocument13 pagesDiagnosis and Classification of Urethral Injuriesleo100% (2)
- Penile Fracture in Spinal Cord InjuryDocument3 pagesPenile Fracture in Spinal Cord InjuryalaaNo ratings yet
- Causes of Penile FractureDocument4 pagesCauses of Penile FracturealaaNo ratings yet
- Dislocation of The PenisDocument3 pagesDislocation of The PenisalaaNo ratings yet
- Penile Fracture & False FractureDocument4 pagesPenile Fracture & False FracturealaaNo ratings yet
- Section A: Select Any 60 Consecutive Multiple Choice Questions. For Each Question Circle One Best AlternativeDocument17 pagesSection A: Select Any 60 Consecutive Multiple Choice Questions. For Each Question Circle One Best AlternativeJeshuah JehopioNo ratings yet
- Male Reproductive SystemDocument152 pagesMale Reproductive SystemRoshan MevadaNo ratings yet
- Assessing Children - Infancy Through Adolescence 1Document118 pagesAssessing Children - Infancy Through Adolescence 1kûrñï såñskrùthîNo ratings yet
- MedCalc Ballard Assessment of Gestational AgeDocument2 pagesMedCalc Ballard Assessment of Gestational AgeYanty DorojatunNo ratings yet
- OrhidopexieDocument7 pagesOrhidopexiediana.miron.mNo ratings yet
- Animal Diary Science 434Document32 pagesAnimal Diary Science 434Luis MenaNo ratings yet
- HYDROCELEDocument2 pagesHYDROCELEKoichi LeeNo ratings yet
- Introduction To Veterinary AnatomyDocument22 pagesIntroduction To Veterinary AnatomyAbdulla Hil KafiNo ratings yet
- USMLE Male Reproductive Disorders 2Document2 pagesUSMLE Male Reproductive Disorders 2kramNo ratings yet
- Undescended Testes: What General Practitioners Need To KnowDocument4 pagesUndescended Testes: What General Practitioners Need To KnowRizka Desti AyuniNo ratings yet
- Urogenital SystemDocument111 pagesUrogenital Systemhamdan hamimNo ratings yet
- Assessment - Nursing Head To ToeDocument14 pagesAssessment - Nursing Head To ToePatria HeberleNo ratings yet
- Penis: Abdomen Skin CircumcisionDocument4 pagesPenis: Abdomen Skin CircumcisionTatadarz Auxtero LagriaNo ratings yet
- No Scalpel PDFDocument70 pagesNo Scalpel PDFSantosh BabuNo ratings yet
- Concealed Penis PDFDocument5 pagesConcealed Penis PDFZlatan ZvizdicNo ratings yet
- Testis Tuberculosis Case Without Pulmonary or Renal InvolvementDocument2 pagesTestis Tuberculosis Case Without Pulmonary or Renal Involvementntambik21No ratings yet
- Case Report: Giant Abdomino Scrotal Hydrocele: A Case Report With Literature ReviewDocument6 pagesCase Report: Giant Abdomino Scrotal Hydrocele: A Case Report With Literature ReviewMella IntaniabellaNo ratings yet
- vùng chậuDocument106 pagesvùng chậuminhmap90_635122804No ratings yet
- Diseases and Disorders of The Male Reproductive SystemDocument16 pagesDiseases and Disorders of The Male Reproductive Systemblythe RiveroNo ratings yet
- Yearling Bull Breeding Soundness ExaminationDocument14 pagesYearling Bull Breeding Soundness ExaminationManu TabarezszNo ratings yet
- # Davalebis Pirobis Adekvaturi Gageba Da Gaazreba Qulebi Adekvaturadaa AraadekvaturadaaDocument4 pages# Davalebis Pirobis Adekvaturi Gageba Da Gaazreba Qulebi Adekvaturadaa AraadekvaturadaaError 404No ratings yet
- Male Genetal OrganDocument7 pagesMale Genetal OrgantomiNo ratings yet
- G10 Science Q3 - Week 1 - Male Reproductive SystemDocument18 pagesG10 Science Q3 - Week 1 - Male Reproductive SystemKlent CalunsagNo ratings yet
- Castration of Large AnimalsDocument17 pagesCastration of Large AnimalsAqsa Zahoor Ahmad NadeemNo ratings yet
- Rep-Jrf 114 2 001Document16 pagesRep-Jrf 114 2 001siyopin173No ratings yet