You might also like
- Sanitation and Hygiene JharkhandDocument44 pagesSanitation and Hygiene JharkhandOscar MoraNo ratings yet
- 2021 Success Stories and Lessons LearnedDocument28 pages2021 Success Stories and Lessons LearnedBerhanu AshebirNo ratings yet
- Faecal Sludge Management ReportDocument180 pagesFaecal Sludge Management ReportfaltuNo ratings yet
- Paliatif WhoDocument72 pagesPaliatif WhoRuwaedaNasruddinNo ratings yet
- Assessing The Development of Palliative Care Worldwide: A Set of Actionable IndicatorsDocument72 pagesAssessing The Development of Palliative Care Worldwide: A Set of Actionable IndicatorsRanga PereraNo ratings yet
- 2016 UNICEF EAPRO WASH Nutrition Toolkit FinalDocument88 pages2016 UNICEF EAPRO WASH Nutrition Toolkit FinalChris ValNo ratings yet
- JMP 2018 Core Questions For Household SurveysDocument24 pagesJMP 2018 Core Questions For Household SurveysNajeebullah MandokhailNo ratings yet
- JMP 2018 Core Questions For Household Surveys PDFDocument24 pagesJMP 2018 Core Questions For Household Surveys PDFKim Alvic Bantilan SaldoNo ratings yet
- Review WASH BATDocument79 pagesReview WASH BATMogesNo ratings yet
- The International Federation Software Tools For Long-Term Water and Sanitation ProgrammingDocument57 pagesThe International Federation Software Tools For Long-Term Water and Sanitation ProgrammingJamalNo ratings yet
- Building On A Decade of Progress in Water, Sanitation and Hygiene To Control, Eliminate and Eradicate Neglected Tropical DiseasesDocument3 pagesBuilding On A Decade of Progress in Water, Sanitation and Hygiene To Control, Eliminate and Eradicate Neglected Tropical DiseasesMstNo ratings yet
- Faecal Sludge Management Landscape in South Asia Synthesis of A Multicountry StudyDocument84 pagesFaecal Sludge Management Landscape in South Asia Synthesis of A Multicountry StudyAmrita AngdembeNo ratings yet
- Water Sanitation and Hygiene in Health Care Facilities Fundamentals First 2020Document164 pagesWater Sanitation and Hygiene in Health Care Facilities Fundamentals First 2020daniah bawazierNo ratings yet
- CWIS ASCI Online Course Cohort 4 Brochure 20 Jan23Document12 pagesCWIS ASCI Online Course Cohort 4 Brochure 20 Jan23Sudhakar KNo ratings yet
- UNICEF - Advancing Children's Rights and Well-Being Through SSTRC (2019)Document54 pagesUNICEF - Advancing Children's Rights and Well-Being Through SSTRC (2019)javedafridiNo ratings yet
- Gender Mainstreaming Impact StudyDocument94 pagesGender Mainstreaming Impact StudyUnited Nations Human Settlements Programme (UN-HABITAT)No ratings yet
- National Hand Hygiene Behaviour Change Strategy - 2016-2020 Final Artwork-Ilovepdf-CompressedDocument48 pagesNational Hand Hygiene Behaviour Change Strategy - 2016-2020 Final Artwork-Ilovepdf-CompressedsmashakeniNo ratings yet
- OMS OIE PHAO PNUMA One-Health-Joint-Plan-Of-Action-Final 2022Document86 pagesOMS OIE PHAO PNUMA One-Health-Joint-Plan-Of-Action-Final 2022francoctf21No ratings yet
- Report 11Document28 pagesReport 11Jyothsna GopisettiNo ratings yet
- WASH GuidelinesDocument133 pagesWASH GuidelinesmoqmerNo ratings yet
- Engagement of Stakeholders in The Development of A Theory of Change For Handwashing and Sanitation Behaviour ChangeDocument16 pagesEngagement of Stakeholders in The Development of A Theory of Change For Handwashing and Sanitation Behaviour ChangeyomnayasminNo ratings yet
- JMP 2016 Annual ReportDocument20 pagesJMP 2016 Annual Reportceking99No ratings yet
- Sanitation HygieneDocument23 pagesSanitation HygieneNayeli Gutiérrez HernándezNo ratings yet
- Issdp 2006-2010Document28 pagesIssdp 2006-2010Bintang Ruth Cecilia FebrinaNo ratings yet
- Hygiene Awareness For Rural Areas in South AfricaDocument3 pagesHygiene Awareness For Rural Areas in South AfricaasgharhamidNo ratings yet
- Addressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)Document48 pagesAddressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)OxfamNo ratings yet
- Addressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)Document48 pagesAddressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)OxfamNo ratings yet
- Addressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)Document48 pagesAddressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)OxfamNo ratings yet
- Addressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)Document48 pagesAddressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)OxfamNo ratings yet
- Addressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)Document48 pagesAddressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)OxfamNo ratings yet
- Addressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)Document48 pagesAddressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)OxfamNo ratings yet
- Addressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)Document48 pagesAddressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)OxfamNo ratings yet
- Addressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)Document48 pagesAddressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)OxfamNo ratings yet
- Addressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)Document48 pagesAddressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)OxfamNo ratings yet
- Addressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)Document48 pagesAddressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)OxfamNo ratings yet
- Addressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)Document48 pagesAddressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)OxfamNo ratings yet
- Addressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)Document48 pagesAddressing Southern Africa's Sanitation Challenges Through Community-Led Total Sanitation (CLTS)OxfamNo ratings yet
- Desal RGDocument168 pagesDesal RGrichu rasheedNo ratings yet
- Drinking Water and Sanitation Part IDocument4 pagesDrinking Water and Sanitation Part ISuiNo ratings yet
- Evaluation of Health, Empowerment, Livelihoods and Protection (HELP) Kailahun Programme in Sierra LeoneDocument50 pagesEvaluation of Health, Empowerment, Livelihoods and Protection (HELP) Kailahun Programme in Sierra LeoneOxfamNo ratings yet
- Xenobiotics and Urban Water: R. Aertgeerts WHO Regional Office For Europe Email: Watsan@ecr - Euro.who - IntDocument27 pagesXenobiotics and Urban Water: R. Aertgeerts WHO Regional Office For Europe Email: Watsan@ecr - Euro.who - IntRizka Dwi AnissatunisaNo ratings yet
- AIHD Annual Report 2010Document45 pagesAIHD Annual Report 2010Monica Wabuke LuttaNo ratings yet
- WSP PeruBaselineStudy HWWSDocument102 pagesWSP PeruBaselineStudy HWWSwsp_scalingupNo ratings yet
- Scaling Up Handwashing Behavior:: Findings From The Impact Evaluation Baseline Survey in SenegalDocument76 pagesScaling Up Handwashing Behavior:: Findings From The Impact Evaluation Baseline Survey in SenegalalexNo ratings yet
- STEWARD WASH Assessment Report June 2013Document152 pagesSTEWARD WASH Assessment Report June 2013Icecold254 IceNo ratings yet
- GLAAS 2017 Report For Web - FinalDocument96 pagesGLAAS 2017 Report For Web - FinalNewsBharatiNo ratings yet
- Spotlight On Handwashing in Rural IndiaDocument52 pagesSpotlight On Handwashing in Rural IndiaPratipal SinghNo ratings yet
- Unicef - Community Led Total SanitationDocument206 pagesUnicef - Community Led Total SanitationElsie JakoNo ratings yet
- Facilitating Active Civic Engagement: From Consultation To ParticipationDocument120 pagesFacilitating Active Civic Engagement: From Consultation To ParticipationOxfamNo ratings yet
- Facilitating Active Civic Engagement: From Consultation To ParticipationDocument120 pagesFacilitating Active Civic Engagement: From Consultation To ParticipationOxfamNo ratings yet
- Facilitating Active Civic Engagement: From Consultation To ParticipationDocument120 pagesFacilitating Active Civic Engagement: From Consultation To ParticipationOxfamNo ratings yet
- Facilitating Active Civic Engagement: From Consultation To ParticipationDocument120 pagesFacilitating Active Civic Engagement: From Consultation To ParticipationOxfamNo ratings yet
- Facilitating Active Civic Engagement: From Consultation To ParticipationDocument120 pagesFacilitating Active Civic Engagement: From Consultation To ParticipationOxfamNo ratings yet
- Facilitating Active Civic Engagement: From Consultation To ParticipationDocument120 pagesFacilitating Active Civic Engagement: From Consultation To ParticipationOxfamNo ratings yet
- Facilitating Active Civic Engagement: From Consultation To ParticipationDocument120 pagesFacilitating Active Civic Engagement: From Consultation To ParticipationOxfamNo ratings yet
- Facilitating Active Civic Engagement: From Consultation To ParticipationDocument120 pagesFacilitating Active Civic Engagement: From Consultation To ParticipationOxfamNo ratings yet
- Facilitating Active Civic Engagement: From Consultation To ParticipationDocument120 pagesFacilitating Active Civic Engagement: From Consultation To ParticipationOxfamNo ratings yet
- Facilitating Active Civic Engagement: From Consultation To ParticipationDocument120 pagesFacilitating Active Civic Engagement: From Consultation To ParticipationOxfamNo ratings yet
- Roof Structure Collapse Report - HongkongDocument11 pagesRoof Structure Collapse Report - HongkongEmdad YusufNo ratings yet
- EC-21.PDF Ranigunj ChamberDocument41 pagesEC-21.PDF Ranigunj ChamberShabbir MoizbhaiNo ratings yet
- Busi Environment MCQDocument15 pagesBusi Environment MCQAnonymous WtjVcZCg57% (7)
- Theodore L. Sendak, Etc. v. Clyde Nihiser, Dba Movieland Drive-In Theater, 423 U.S. 976 (1975)Document4 pagesTheodore L. Sendak, Etc. v. Clyde Nihiser, Dba Movieland Drive-In Theater, 423 U.S. 976 (1975)Scribd Government DocsNo ratings yet
- Chap 2 Human Resource Strategy and PerformanceDocument35 pagesChap 2 Human Resource Strategy and PerformanceĐinh HiệpNo ratings yet
- Executive Summary: College of EngineeringDocument17 pagesExecutive Summary: College of Engineeringjoel c. herreraNo ratings yet
- 1 Rodney Britton v. Apple Inc. Job Descrimination, Sexual HarrassmentDocument8 pages1 Rodney Britton v. Apple Inc. Job Descrimination, Sexual HarrassmentJack PurcherNo ratings yet
- S0260210512000459a - CamilieriDocument22 pagesS0260210512000459a - CamilieriDanielNo ratings yet
- Warhammer Armies: The Army of The NorseDocument39 pagesWarhammer Armies: The Army of The NorseAndy Kirkwood100% (2)
- Farhat Ziadeh - Winds Blow Where Ships Do Not Wish To GoDocument32 pagesFarhat Ziadeh - Winds Blow Where Ships Do Not Wish To GoabshlimonNo ratings yet
- Japanese Erotic Fantasies: Sexual Imagery of The Edo PeriodDocument12 pagesJapanese Erotic Fantasies: Sexual Imagery of The Edo Periodcobeboss100% (4)
- Us and China Trade WarDocument2 pagesUs and China Trade WarMifta Dian Pratiwi100% (1)
- Top Notch 1 Unit 9 AssessmentDocument6 pagesTop Notch 1 Unit 9 AssessmentMa Camila Ramírez50% (6)
- Yellow Submarine - Amended Case Study - Final Written Report - Group 4Document12 pagesYellow Submarine - Amended Case Study - Final Written Report - Group 4Kristine Diones100% (1)
- ConsignmentDocument2 pagesConsignmentKanniha SuryavanshiNo ratings yet
- Sample of Notarial WillDocument3 pagesSample of Notarial WillJF Dan100% (1)
- Suffolk County Substance Abuse ProgramsDocument44 pagesSuffolk County Substance Abuse ProgramsGrant ParpanNo ratings yet
- Breterg RSGR: Prohibition Against CarnalityDocument5 pagesBreterg RSGR: Prohibition Against CarnalityemasokNo ratings yet
- Methodology For Rating General Trading and Investment CompaniesDocument23 pagesMethodology For Rating General Trading and Investment CompaniesAhmad So MadNo ratings yet
- People Vs Gonzales-Flores - 138535-38 - April 19, 2001 - JDocument10 pagesPeople Vs Gonzales-Flores - 138535-38 - April 19, 2001 - JTrexPutiNo ratings yet
- Spiritual Fitness Assessment: Your Name: - Date: - InstructionsDocument2 pagesSpiritual Fitness Assessment: Your Name: - Date: - InstructionsLeann Kate MartinezNo ratings yet
- Why Study in USADocument4 pagesWhy Study in USALowlyLutfurNo ratings yet
- Taller InglesDocument11 pagesTaller InglesMartín GonzálezNo ratings yet
- A Wolf by The Ears - Mattie LennonDocument19 pagesA Wolf by The Ears - Mattie LennonMirNo ratings yet
- Gabbard - Et - Al - The Many Faces of Narcissism 2016-World - Psychiatry PDFDocument2 pagesGabbard - Et - Al - The Many Faces of Narcissism 2016-World - Psychiatry PDFatelierimkellerNo ratings yet
- 13th Format SEX Format-1-1: Share This DocumentDocument1 page13th Format SEX Format-1-1: Share This DocumentDove LogahNo ratings yet
- 1 PDFDocument176 pages1 PDFDigna Bettin CuelloNo ratings yet
- Quality Audit Report TemplateDocument3 pagesQuality Audit Report TemplateMercy EdemNo ratings yet
- Mandatory Minimum Requirements For Security-Related Training and Instruction For All SeafarersDocument9 pagesMandatory Minimum Requirements For Security-Related Training and Instruction For All SeafarersDio Romero FariaNo ratings yet
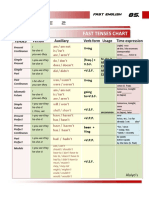
- Table 2: Fast Tenses ChartDocument5 pagesTable 2: Fast Tenses ChartAngel Julian HernandezNo ratings yet