You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- 89Document7 pages89Beatriz ChilenoNo ratings yet
- RX Sheet Indirect Bonding PDFDocument1 pageRX Sheet Indirect Bonding PDFBeatriz ChilenoNo ratings yet
- Evolution of Treatment Mechanics and Contemporary Appliance Design in Orthodontics: A 40-Year PerspectiveDocument9 pagesEvolution of Treatment Mechanics and Contemporary Appliance Design in Orthodontics: A 40-Year PerspectiveBeatriz ChilenoNo ratings yet
- A Longitudinal Evaluation of Extraction Versus Nonextraction Treatment With Special Reference To The Posttreatment Irregularity of The Lower IncisorsDocument11 pagesA Longitudinal Evaluation of Extraction Versus Nonextraction Treatment With Special Reference To The Posttreatment Irregularity of The Lower IncisorsBeatriz ChilenoNo ratings yet
- Bousquet 2006Document6 pagesBousquet 2006Beatriz ChilenoNo ratings yet
- Offline List GrowthDocument8 pagesOffline List GrowthBeatriz ChilenoNo ratings yet
- Barlow 2008Document9 pagesBarlow 2008Beatriz ChilenoNo ratings yet
- Comparison of Two Protocols For Maxillary Protraction: Bone Anchors Versus Face Mask With Rapid Maxillary ExpansionDocument8 pagesComparison of Two Protocols For Maxillary Protraction: Bone Anchors Versus Face Mask With Rapid Maxillary ExpansionBeatriz ChilenoNo ratings yet
- Pigment Effect On The Long Term Elasticity of Elastomeric LigaturesDocument6 pagesPigment Effect On The Long Term Elasticity of Elastomeric LigaturesBeatriz ChilenoNo ratings yet
- Efficacy of Orthopedic Treatment With Protraction Facemask On Skeletal Class III Malocclusion: A Systematic Review and Meta-AnalysisDocument11 pagesEfficacy of Orthopedic Treatment With Protraction Facemask On Skeletal Class III Malocclusion: A Systematic Review and Meta-AnalysisnhasuonlineNo ratings yet
- Inclinacion Incisiva PerfilDocument9 pagesInclinacion Incisiva PerfilBeatriz ChilenoNo ratings yet
- Class III High Angle Malocclusion Treated With Orthodontic Camouflage (MEAW Therapy)Document24 pagesClass III High Angle Malocclusion Treated With Orthodontic Camouflage (MEAW Therapy)Beatriz ChilenoNo ratings yet
- Eliades 2007Document10 pagesEliades 2007Beatriz ChilenoNo ratings yet
- G Developdentition PDFDocument13 pagesG Developdentition PDFZita AprilliaNo ratings yet
- American Journal of ORTHODONTICS and Dentofacial OrthopedicsDocument11 pagesAmerican Journal of ORTHODONTICS and Dentofacial OrthopedicsBeatriz ChilenoNo ratings yet
- Bousquet 2006Document6 pagesBousquet 2006Beatriz ChilenoNo ratings yet
- Research Journal of Pharmaceutical, Biological and Chemical SciencesDocument6 pagesResearch Journal of Pharmaceutical, Biological and Chemical SciencesBeatriz ChilenoNo ratings yet
- 6 RossDocument2 pages6 RossBeatriz ChilenoNo ratings yet
- 10 HauserDocument4 pages10 HauserBeatriz ChilenoNo ratings yet
- Management of Midline Facial CleftsDocument8 pagesManagement of Midline Facial CleftsBeatriz ChilenoNo ratings yet
- Plano Oclusal y SonrisaDocument6 pagesPlano Oclusal y SonrisaBeatriz ChilenoNo ratings yet
- Et DX y Manejo OrtoDocument6 pagesEt DX y Manejo OrtoBeatriz ChilenoNo ratings yet
- 16 TauscheDocument9 pages16 TauscheBeatriz ChilenoNo ratings yet
- Asimetrias Borde IncisalDocument7 pagesAsimetrias Borde IncisalBeatriz ChilenoNo ratings yet
- Pi Is 0889540614009299Document8 pagesPi Is 0889540614009299Beatriz ChilenoNo ratings yet
- En V26n4a15Document7 pagesEn V26n4a15Beatriz ChilenoNo ratings yet
- CleftLipandPalate2Read OnlyDocument16 pagesCleftLipandPalate2Read OnlyBeatriz ChilenoNo ratings yet
- Early Craniofacial Morphology and Growth in Children With Bilateral Complete Cleft Lip and PalateDocument15 pagesEarly Craniofacial Morphology and Growth in Children With Bilateral Complete Cleft Lip and PalateBeatriz ChilenoNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Job Description: University College London Hospitals NHS Foundation TrustDocument13 pagesJob Description: University College London Hospitals NHS Foundation TrustM LubisNo ratings yet
- The Novice Nurse's Guide To Calling "Code Blue": Wayne Thomas Brice, MA, RN-BCDocument5 pagesThe Novice Nurse's Guide To Calling "Code Blue": Wayne Thomas Brice, MA, RN-BCniraNo ratings yet
- RH IncompatibilityDocument22 pagesRH IncompatibilityDrPreeti Thakur ChouhanNo ratings yet
- Peripheral IntravenousDocument12 pagesPeripheral IntravenousDewi List0% (1)
- HPNDocument3 pagesHPNFerdyNo ratings yet
- O&g Case Write UpDocument17 pagesO&g Case Write Upmohd faizhakimNo ratings yet
- Case 3:myopiaDocument24 pagesCase 3:myopiaarifamri92No ratings yet
- Gross Anatomy Urinary SystemDocument43 pagesGross Anatomy Urinary SystemMay LacdaoNo ratings yet
- CVDocument8 pagesCVJuan Rafael SilvaNo ratings yet
- Scale Down of Services Port Moresby General Hospital 17 Jul 2020Document2 pagesScale Down of Services Port Moresby General Hospital 17 Jul 2020csgo mainNo ratings yet
- Action Plan of Directorate of Central Health EstablishmentDocument1 pageAction Plan of Directorate of Central Health EstablishmentDirectorate of Central Health EstablishmentsNo ratings yet
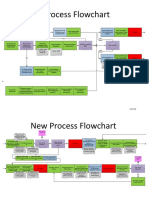
- New Process Flowchart CPOEDocument4 pagesNew Process Flowchart CPOELiza GeorgeNo ratings yet
- Article - Self-Scheduling For Hospital NursesDocument6 pagesArticle - Self-Scheduling For Hospital NursesDavidNo ratings yet
- Management of Pediatric Femoral Neck FractureDocument21 pagesManagement of Pediatric Femoral Neck FracturevikidwirandaNo ratings yet
- Nephrolithiasis AnatomyDocument3 pagesNephrolithiasis AnatomyKevin Ker Campaner MerillesNo ratings yet
- Medical Terms (Prefixes Suffixes Roots)Document5 pagesMedical Terms (Prefixes Suffixes Roots)David Donovan ManuelNo ratings yet
- Show Mom HowDocument20 pagesShow Mom HowWeldon Owen Publishing75% (4)
- Traction in Orthopaedics - Mus'Document72 pagesTraction in Orthopaedics - Mus'Muslihah Zainon100% (1)
- Programa Aua San Francisco 2018Document76 pagesPrograma Aua San Francisco 2018Rosemary FranquizNo ratings yet
- CSR Initiatives by Welspun FINALDocument24 pagesCSR Initiatives by Welspun FINALRitesh RamanNo ratings yet
- Size GeneticsDocument7 pagesSize Geneticsraspberry54321No ratings yet
- Iron Deficiency Anemia Among Pregnant Women in Nablus District Prevalence Knowledge Attitude and Practices PDFDocument72 pagesIron Deficiency Anemia Among Pregnant Women in Nablus District Prevalence Knowledge Attitude and Practices PDFEArl CopinaNo ratings yet
- Flyer SugiesDocument2 pagesFlyer SugiesInomy ClaudiaNo ratings yet
- Ovarian TorsionDocument4 pagesOvarian TorsionRiko KuswaraNo ratings yet
- Rekomendasi Antibiotik Pada Profilaksis BedahDocument4 pagesRekomendasi Antibiotik Pada Profilaksis BedahRya At ChinnamorariaNo ratings yet
- Diagnosing Anemia in Neonates An Evidence-Based ApproachDocument13 pagesDiagnosing Anemia in Neonates An Evidence-Based Approacharmando salvador100% (1)
- Genre Paper DraftDocument5 pagesGenre Paper Draftapi-241693751No ratings yet
- PPIUDDocument16 pagesPPIUDmusicwizardNo ratings yet
- Eng Philosophy and Model of Midwifery CareDocument4 pagesEng Philosophy and Model of Midwifery CareJefrioSuyantoNo ratings yet
- Hernia Surgeon in Pune - DR Sanjay KolteDocument12 pagesHernia Surgeon in Pune - DR Sanjay KolteRushiNo ratings yet