You might also like
- Research in Psychotherapy and CounsellingFrom EverandResearch in Psychotherapy and CounsellingRating: 3 out of 5 stars3/5 (3)
- Solution-Focused Brief Therapy: Chris IvesonDocument9 pagesSolution-Focused Brief Therapy: Chris IvesonAnonymous 9yIlDrElz7No ratings yet
- Research Paper On Motivational InterviewingDocument7 pagesResearch Paper On Motivational Interviewingafeaxbgqp100% (1)
- First Session Solution-Focused Brief Therapy With PDFDocument24 pagesFirst Session Solution-Focused Brief Therapy With PDFMasniahNo ratings yet
- Applications of Solution-Focused Brief Therapy in Suicide Prevention PDFDocument13 pagesApplications of Solution-Focused Brief Therapy in Suicide Prevention PDFsolutions4familyNo ratings yet
- CLIENT VARIABLES and Psychotherapy OutcomesDocument20 pagesCLIENT VARIABLES and Psychotherapy OutcomespsicandreiaNo ratings yet
- Overrating or Dismissing The Value of Evidence-Based Practice+++Document7 pagesOverrating or Dismissing The Value of Evidence-Based Practice+++pig5evans30No ratings yet
- Clinical Reasoning in Psychosocial Occupational Therapy - The Evaluation Process. Barris1987Document16 pagesClinical Reasoning in Psychosocial Occupational Therapy - The Evaluation Process. Barris1987saraNo ratings yet
- Contemporary Theory and Practice in Counseling and Psychotherapy - I2949Document26 pagesContemporary Theory and Practice in Counseling and Psychotherapy - I2949Michelle KellyNo ratings yet
- Research Paper On Solution-focused-TherapyDocument8 pagesResearch Paper On Solution-focused-Therapylzpyreqhf100% (1)
- Effectiveness Study Article On Psychodynamic PsychotherapyDocument10 pagesEffectiveness Study Article On Psychodynamic PsychotherapyRiham AmmarNo ratings yet
- Solution-Focused Brief Therapy and Motivational Interviewing Aarya MathewDocument47 pagesSolution-Focused Brief Therapy and Motivational Interviewing Aarya MathewAarya MathewNo ratings yet
- HSER511 EthicsPaperDocument19 pagesHSER511 EthicsPaperAnna Baucum ChapmanNo ratings yet
- Improve Your Therapeutic Effi CT IvenessDocument29 pagesImprove Your Therapeutic Effi CT IvenessSushil AcharyaNo ratings yet
- The Elements of Effective Counselling - NATCONDocument9 pagesThe Elements of Effective Counselling - NATCONHugomarNo ratings yet
- Pluralism, Diversity, and Sophistication in Family Therapy ResearchDocument16 pagesPluralism, Diversity, and Sophistication in Family Therapy ResearchUmi NurhidayahNo ratings yet
- 2011 O'HanlonDocument16 pages2011 O'HanlonPsicóloga Lily CavazosNo ratings yet
- The Journey of The Counselor and Therapist: Research Findings and Perspectives On Professional DevelopmentDocument40 pagesThe Journey of The Counselor and Therapist: Research Findings and Perspectives On Professional DevelopmentPyan DaffaNo ratings yet
- Solution Focused Therapy Revised - Treatment - Manual - 2013 PDFDocument42 pagesSolution Focused Therapy Revised - Treatment - Manual - 2013 PDFAriel Pollak67% (3)
- Bond Et Al. (2013) Practitioner Review - The Effectiveness of Solution Focused Brief Therapy With Children and Families - A Systematic and Critical Evaluation of The Literature From 1990-2010Document17 pagesBond Et Al. (2013) Practitioner Review - The Effectiveness of Solution Focused Brief Therapy With Children and Families - A Systematic and Critical Evaluation of The Literature From 1990-2010sofiaNo ratings yet
- Solution Focused Therapy 9Document18 pagesSolution Focused Therapy 9Mirela Cojocaru StetcoNo ratings yet
- Solution-Focused Brief Therapy With Long-Term ProblemsDocument11 pagesSolution-Focused Brief Therapy With Long-Term ProblemsGustavo Paniagua100% (1)
- Solution Focused Brief Therapy - FINALDocument14 pagesSolution Focused Brief Therapy - FINALbose balogunNo ratings yet
- What Do Others Think The Why When and How of Using Surveys in CBTDocument11 pagesWhat Do Others Think The Why When and How of Using Surveys in CBTANGELICANo ratings yet
- Solution Focused With AdolescentsDocument28 pagesSolution Focused With AdolescentsAlina Purdea100% (1)
- FACT Kirk Strosahl Presentation PDFDocument11 pagesFACT Kirk Strosahl Presentation PDFAlexander ZelenukhinNo ratings yet
- Journal Club 4: Intervention StudiesDocument4 pagesJournal Club 4: Intervention StudiesSpeech & Language Therapy in PracticeNo ratings yet
- Occupational Therapy Thesis ExamplesDocument7 pagesOccupational Therapy Thesis Examplesdwpeprje100% (2)
- When Therapy Causes HarmDocument3 pagesWhen Therapy Causes HarmJose Oso SosaNo ratings yet
- Change Process Research in PsychotherapyDocument19 pagesChange Process Research in PsychotherapyJuanaNo ratings yet
- 2002 Solution-Focused Brief TherapyDocument9 pages2002 Solution-Focused Brief Therapymgnpni100% (1)
- The Dance of Empathy - Empathy, Diversity, Technical Eclecticism - Bohart, Arthur C. & Rosenbaum, RobertDocument24 pagesThe Dance of Empathy - Empathy, Diversity, Technical Eclecticism - Bohart, Arthur C. & Rosenbaum, RobertBotezat-AntonescuRaduAndreiNo ratings yet
- Sesión 1. Uncovering MRI Roots en Solution Therapy LipchikDocument7 pagesSesión 1. Uncovering MRI Roots en Solution Therapy LipchikAna María González FNo ratings yet
- Therapists Views On The Use of Questions in PersoDocument14 pagesTherapists Views On The Use of Questions in PersoNorus LizaNo ratings yet
- The Effects of Fifteen Evidence-Supported Therapies For Adult Depress...Document16 pagesThe Effects of Fifteen Evidence-Supported Therapies For Adult Depress...Nicolas GeniseNo ratings yet
- Appi Psychotherapy 2006 60 2 147Document6 pagesAppi Psychotherapy 2006 60 2 147João PerestreloNo ratings yet
- Occupational Therapy Research Paper TopicsDocument6 pagesOccupational Therapy Research Paper Topicsc9kb0esz100% (1)
- Clinical FormulationDocument24 pagesClinical Formulationaimee2oo8100% (2)
- Artand Scienceof Asking Questionsin CBTDocument21 pagesArtand Scienceof Asking Questionsin CBTVaaniNo ratings yet
- Solution Focused TherapyDocument7 pagesSolution Focused TherapyAditi KirtaneNo ratings yet
- Theory and Clinical ApplicationDocument22 pagesTheory and Clinical ApplicationGosia GratefulNo ratings yet
- Seligman 1995 PDFDocument10 pagesSeligman 1995 PDFEdy WallerNo ratings yet
- Evidence Based Treatment: What Is It and How Can It Help ChildrenDocument27 pagesEvidence Based Treatment: What Is It and How Can It Help ChildrenJohn Gavazzi100% (1)
- The Therapist A Neglected Variable in Psychotherapy ResearchDocument4 pagesThe Therapist A Neglected Variable in Psychotherapy ResearchPaulo GomesNo ratings yet
- Focusing On Therapists in Co-Research Interviews: How Do Therapists See Couple Therapy?Document22 pagesFocusing On Therapists in Co-Research Interviews: How Do Therapists See Couple Therapy?Alexandra CatalinaNo ratings yet
- Carl Rogers 1Document10 pagesCarl Rogers 1Monica S. SantiagoNo ratings yet
- Evidencebase TherapyDocument13 pagesEvidencebase TherapyToolika W100% (1)
- Beyebachetal 1996Document37 pagesBeyebachetal 1996zeinabNo ratings yet
- Justify The Relevance of Research Work at The WorkplaceDocument6 pagesJustify The Relevance of Research Work at The WorkplaceTendaiNo ratings yet
- Counseling Theory Case Study Application 1Document10 pagesCounseling Theory Case Study Application 1Sushma karkiNo ratings yet
- Therapeutic Assessment Untuk Di Review Oleh Mahasiswa Secara IndividuDocument4 pagesTherapeutic Assessment Untuk Di Review Oleh Mahasiswa Secara IndividunadiyaNo ratings yet
- Using Microanalysis of Communication To Compare Solution-Focused and Client-Centered Therapies Christine Tomori Janet Beavin Bavela 2007 To Moriba VelasDocument10 pagesUsing Microanalysis of Communication To Compare Solution-Focused and Client-Centered Therapies Christine Tomori Janet Beavin Bavela 2007 To Moriba VelasSandy ThedabNo ratings yet
- Factors For Personal CounselingDocument12 pagesFactors For Personal CounselingRashika JayakumarNo ratings yet
- Winds of Change For Client-Centered Therapy - Patterson C. H.Document15 pagesWinds of Change For Client-Centered Therapy - Patterson C. H.Botezat-AntonescuRaduAndreiNo ratings yet
- Solution 20 Focused 20 Career 20 HelpDocument16 pagesSolution 20 Focused 20 Career 20 HelpAmy Rowan Hartin100% (1)
- Solution-Focused Family TherapyDocument15 pagesSolution-Focused Family Therapyltlmiss100% (8)
- 3 Solution Focused TherapyDocument17 pages3 Solution Focused TherapyEllia WatersNo ratings yet
- Integrative Brief Solution-Focused Family Therapy A Provisional Roadmap PDFDocument19 pagesIntegrative Brief Solution-Focused Family Therapy A Provisional Roadmap PDFRocio ANo ratings yet
- Solution Focused Brief TherapyDocument20 pagesSolution Focused Brief TherapyKaye Peralta100% (6)
- Working With Mandated Substance Abusers - Language of SolutionsDocument33 pagesWorking With Mandated Substance Abusers - Language of SolutionsbmckNo ratings yet
- SMART Recovery-Based Goal and Action-Setting SpecificDocument1 pageSMART Recovery-Based Goal and Action-Setting SpecificbmckNo ratings yet
- How User-Friendly Are Our Tools?: Ideas/suggestion To Improve ScoreDocument1 pageHow User-Friendly Are Our Tools?: Ideas/suggestion To Improve ScorebmckNo ratings yet
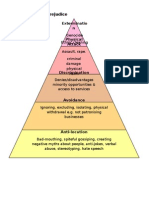
- Allports Scale of PrejudiceDocument1 pageAllports Scale of PrejudicebmckNo ratings yet
- Brown and Blue and GreekDocument106 pagesBrown and Blue and Greektranti100% (1)
- Week#1 - 3. Better - Learning - BloomDocument14 pagesWeek#1 - 3. Better - Learning - BloomTPO MCERCNo ratings yet
- Final Placement Goals-2Document1 pageFinal Placement Goals-2api-466552053No ratings yet
- Latonya's Teaching StatementDocument2 pagesLatonya's Teaching Statementlatonya millienNo ratings yet
- Reviewer For CNU Social SciencesDocument97 pagesReviewer For CNU Social SciencesCARL KENNETH CARINGALNo ratings yet
- Final Week 7 Eng 5Document4 pagesFinal Week 7 Eng 5Bencea CoronadoNo ratings yet
- Architectural Journalism - A View PointDocument2 pagesArchitectural Journalism - A View PointShaurya Chauhan100% (3)
- Claim Evidence Reasoning RubricDocument1 pageClaim Evidence Reasoning Rubricapi-388283259No ratings yet
- DLL - Science 6 - Q2 - W8Document5 pagesDLL - Science 6 - Q2 - W8jerwin remocal100% (1)
- Intercultural Communication Globalization and Social Justice (Kathryn Sorrells)Document444 pagesIntercultural Communication Globalization and Social Justice (Kathryn Sorrells)Omar Leon IñiguezNo ratings yet
- Literacy Mini LessonDocument4 pagesLiteracy Mini LessonSteffaneyNo ratings yet
- JEE (Main) AcknowledgementPageDocument1 pageJEE (Main) AcknowledgementPageAjeet KumarNo ratings yet
- David Koyzis - Dooyeweerd RevisedDocument21 pagesDavid Koyzis - Dooyeweerd RevisedLeonardoAmaralNo ratings yet
- Electronic Ranking Form 1.0 (8 Subjects)Document4 pagesElectronic Ranking Form 1.0 (8 Subjects)PEDRITO DULAYNo ratings yet
- ABUBAKAR Clearance and Eligibility Form OldDocument2 pagesABUBAKAR Clearance and Eligibility Form OldBello KellyNo ratings yet
- GED 109 Research - List of ArticlesDocument2 pagesGED 109 Research - List of ArticlesJeazelle RuazolNo ratings yet
- Masood - Administrative CapitalDocument17 pagesMasood - Administrative CapitalMaimarinhoNo ratings yet
- Resume Preya Del MundoDocument3 pagesResume Preya Del MundoPrecious Del mundoNo ratings yet
- Nursing Program at LangaraDocument6 pagesNursing Program at LangaraHardeeshNo ratings yet
- 1997 - Shaughnessy 1997Document17 pages1997 - Shaughnessy 1997Nathalia Morgado HdzNo ratings yet
- eNGLISH SUMMATIVE TESTDocument2 pageseNGLISH SUMMATIVE TESTLEILANIE ABADNo ratings yet
- Appolo TyresDocument98 pagesAppolo TyresGobind Cj100% (3)
- Clinical FocusDocument9 pagesClinical FocusRobin Halili100% (2)
- History of Health EducationDocument9 pagesHistory of Health EducationJamie Rose FontanillaNo ratings yet
- Abundis Mendivil Sofía Getting Things DoneDocument6 pagesAbundis Mendivil Sofía Getting Things DoneSof AMNo ratings yet
- Handbook For Enhancing Professional Practice - Chapter 1 - EvidenceDocument12 pagesHandbook For Enhancing Professional Practice - Chapter 1 - EvidenceAdvanceIllinois100% (1)
- Equality of Educational Opportunity?: A Look at Social Class Differences and InequalitiesDocument19 pagesEquality of Educational Opportunity?: A Look at Social Class Differences and InequalitiesNivedita RaiNo ratings yet
- The Lamppost: Important DatesDocument8 pagesThe Lamppost: Important DatesleconteschoolNo ratings yet
- Parent Education in The Suzuki Method - Método SuzukiDocument28 pagesParent Education in The Suzuki Method - Método SuzukiWordsandMusic100% (1)
- DV Resume 1Document2 pagesDV Resume 1api-347364550No ratings yet