You might also like
- Pulp Protection AgentsDocument59 pagesPulp Protection Agentsتامي المغربيNo ratings yet
- Cavity Liner, Base and Varnish SanteDocument68 pagesCavity Liner, Base and Varnish Santekali natiNo ratings yet
- Cement Bases and Cavity Liners LectureDocument8 pagesCement Bases and Cavity Liners Lectureمحمد احمد محمدNo ratings yet
- Cement Bases LinersDocument50 pagesCement Bases LinersNoura RihanNo ratings yet
- Cements and Adhesives in Orthodontics - An Update: January 2012Document7 pagesCements and Adhesives in Orthodontics - An Update: January 2012ReshamIrshadNo ratings yet
- Cemento Dental 3mDocument28 pagesCemento Dental 3malecnop52No ratings yet
- Clinical Performance of Glass IonomerDocument8 pagesClinical Performance of Glass Ionomerblue nNo ratings yet
- Cementation of Indirect Restorations - An Overview of Resin CementsDocument6 pagesCementation of Indirect Restorations - An Overview of Resin CementsNaoki MezarinaNo ratings yet
- DR Sonu (Cements)Document123 pagesDR Sonu (Cements)SonuNo ratings yet
- CementsandadhesveDocument7 pagesCementsandadhesveNAHLA ELKHOLYNo ratings yet
- DENTMATCementsDocument3 pagesDENTMATCementsHannah RosalesNo ratings yet
- All DMS Essay Questions 06-14Document17 pagesAll DMS Essay Questions 06-14mepegajNo ratings yet
- Cements For Use in Esthetic DentistryDocument19 pagesCements For Use in Esthetic DentistryMohammed AldaosariNo ratings yet
- Dental Cements: Zinc PhosphateDocument5 pagesDental Cements: Zinc PhosphatetzuquinoNo ratings yet
- Composite ResinDocument26 pagesComposite ResinKhylle Camron LuzzieNo ratings yet
- LINERS AND BASES FOR PULP PROTECTIONDocument92 pagesLINERS AND BASES FOR PULP PROTECTIONpranaliNo ratings yet
- A Review of Luting AgentsDocument8 pagesA Review of Luting AgentsNada EmadNo ratings yet
- How the longevity of fixed dental prostheses depends on the cement functionDocument12 pagesHow the longevity of fixed dental prostheses depends on the cement functionYusuf DiansyahNo ratings yet
- 04 - 003 Dental Luting CementsDocument2 pages04 - 003 Dental Luting CementsZazilatul KhikmiahNo ratings yet
- A Review of Dental Cements: Kipp Wingo, DVM, DAVDCDocument10 pagesA Review of Dental Cements: Kipp Wingo, DVM, DAVDCSaad LiaqatNo ratings yet
- 7 - DrAbeer's Lecture (Dental Cements & Cementation Procedures) PDFDocument51 pages7 - DrAbeer's Lecture (Dental Cements & Cementation Procedures) PDFTasneem ShamaliNo ratings yet
- Technical Product Profile: RelyxDocument28 pagesTechnical Product Profile: RelyxTriawan NuswantoroNo ratings yet
- Non-adhesive cement cannot bond to tooth structure or restoration. Resin cement bonds micromechanically to etched surfacesDocument89 pagesNon-adhesive cement cannot bond to tooth structure or restoration. Resin cement bonds micromechanically to etched surfacesNikita Aggarwal71% (7)
- Operative Chapter 12 Intermediary Liners and BasesDocument14 pagesOperative Chapter 12 Intermediary Liners and BasesNasser HashimNo ratings yet
- MINIMAL iNTERVENTION CARIOLOGYDocument2 pagesMINIMAL iNTERVENTION CARIOLOGYJose Ignacio ZalbaNo ratings yet
- 04 - 003 Dental Luting CementsDocument2 pages04 - 003 Dental Luting CementskaniaNo ratings yet
- Material Merged MergedDocument204 pagesMaterial Merged MergedBasma BasemNo ratings yet
- 2 - CementNotes2022-23Document7 pages2 - CementNotes2022-23Rana hasanaNo ratings yet
- Self-Etch Approach (Etch-and-Dry) : 1 - Classification According To TheirDocument8 pagesSelf-Etch Approach (Etch-and-Dry) : 1 - Classification According To Theirmohamed saadNo ratings yet
- Glass IonomerDocument4 pagesGlass Ionomermaytee19No ratings yet
- Dental CementDocument74 pagesDental CementAisha samreenNo ratings yet
- Varnishes Liners BasesDocument35 pagesVarnishes Liners BasesAbdul ShameemNo ratings yet
- Proper selection of dental cementsDocument6 pagesProper selection of dental cementsNabilah NazalikaNo ratings yet
- Luting Agents PDFDocument13 pagesLuting Agents PDFSandeep VermaNo ratings yet
- Dental JOURNAL: New Era in Denture Base Resins: A ReviewDocument8 pagesDental JOURNAL: New Era in Denture Base Resins: A Reviewpriyanka shelkeNo ratings yet
- LO1Document4 pagesLO1Sidra NurulNo ratings yet
- Pulp ProtectionDocument4 pagesPulp ProtectionNaji Z. Arandi0% (1)
- Estethic Direct Restorative MaterialDocument32 pagesEstethic Direct Restorative MaterialdermagaNo ratings yet
- Luting Agents and Cementation Techniques: April 2021Document11 pagesLuting Agents and Cementation Techniques: April 2021Anh Tuan DangNo ratings yet
- Relyx UnicemDocument40 pagesRelyx Unicemirish.hepiNo ratings yet
- Esthetic Restorative Materials 5Document1 pageEsthetic Restorative Materials 5Tayyuba AslamNo ratings yet
- Introduction to Restorations, Luting and Pulp TherapyDocument11 pagesIntroduction to Restorations, Luting and Pulp TherapyArchanaNo ratings yet
- Operative 20 VeneersDocument21 pagesOperative 20 VeneersInneke SutantoNo ratings yet
- Resin Modified Glass Ionomer Cement: The Holy Grail of Cements?Document3 pagesResin Modified Glass Ionomer Cement: The Holy Grail of Cements?DentalLearningNo ratings yet
- All Ceramic Cementation A Key To Successful RestorationDocument9 pagesAll Ceramic Cementation A Key To Successful RestorationJUDITH ESTHER HIGUERA MESANo ratings yet
- A Literature Review On Selection of Dental Cement in DentistryDocument3 pagesA Literature Review On Selection of Dental Cement in DentistrygeovaniNo ratings yet
- Self-etch Adhesive Classification and Bonding MechanismsDocument5 pagesSelf-etch Adhesive Classification and Bonding Mechanismsmohamed saadNo ratings yet
- Dentmat FinalsDocument14 pagesDentmat Finalslesterliclican22No ratings yet
- Selecting The Right Cement For: Restoration SuccessDocument9 pagesSelecting The Right Cement For: Restoration SuccessLuciano JesusNo ratings yet
- Dental Cements: BY Pranalika Kanojiya Mds 1 YearDocument128 pagesDental Cements: BY Pranalika Kanojiya Mds 1 Yearpranalika .................No ratings yet
- Adhesion and Dentin Bonding AgentsDocument50 pagesAdhesion and Dentin Bonding AgentsFatema86100% (2)
- 4º Articulo Cementation of Indirect RestorationsDocument6 pages4º Articulo Cementation of Indirect RestorationsERIKA BLANQUETNo ratings yet
- Try in FPDDocument40 pagesTry in FPDharshini100% (1)
- Pulp Protection Methods and MaterialsDocument13 pagesPulp Protection Methods and MaterialsmirfanulhaqNo ratings yet
- Pulp Protection Methods and MaterialsDocument13 pagesPulp Protection Methods and MaterialsmirfanulhaqNo ratings yet
- Comparative Evaluation of The Diametral Tensile Strength of Four Commercially Available Luting Cements An in - Vitro StudyDocument16 pagesComparative Evaluation of The Diametral Tensile Strength of Four Commercially Available Luting Cements An in - Vitro StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cement Ebook Layout 3.8.19 PDFDocument27 pagesCement Ebook Layout 3.8.19 PDFIndira Mota100% (1)
- Nbde IiDocument73 pagesNbde IiMarisa Deana Pontrelli100% (1)
- Materials For Direct RestorationsDocument9 pagesMaterials For Direct RestorationsBerty SusantoNo ratings yet
- Jced 10 E75Document6 pagesJced 10 E75bkprosthoNo ratings yet
- Cods 9 41 PDFDocument5 pagesCods 9 41 PDFSweet SumanNo ratings yet
- Bda Cross InfectionDocument6 pagesBda Cross InfectionbkprosthoNo ratings yet
- Dent Update 2004 31 305-306Document3 pagesDent Update 2004 31 305-306bkprosthoNo ratings yet
- Management of Primary Failures Related To Fixed Metal Ceramic Bridge Prosthesis Made by Dental StudentsDocument4 pagesManagement of Primary Failures Related To Fixed Metal Ceramic Bridge Prosthesis Made by Dental Studentsbkprostho0% (1)
- Alzheimer's Disease and Oral CareDocument5 pagesAlzheimer's Disease and Oral CarebkprosthoNo ratings yet
- Infection Control Procedures in Commercial Dental Laboratories in JordanDocument5 pagesInfection Control Procedures in Commercial Dental Laboratories in JordanbkprosthoNo ratings yet
- Clinical Attitude For Failed Fixed Restorations An Overview DOJ 2 119Document5 pagesClinical Attitude For Failed Fixed Restorations An Overview DOJ 2 119Aatish Dilip ShahNo ratings yet
- Understanding Problems and Failures in TSFDP: Peer Review StatusDocument7 pagesUnderstanding Problems and Failures in TSFDP: Peer Review StatusbkprosthoNo ratings yet
- 1801cei Bernie Web PDFDocument10 pages1801cei Bernie Web PDFbkprosthoNo ratings yet
- Infection PreventionDocument48 pagesInfection PreventionbkprosthoNo ratings yet
- Bda Cross Infection PDFDocument21 pagesBda Cross Infection PDFFiona Febriyanti CiamanNo ratings yet
- Jaw Relation Records Guide Fixed ProsthodonticsDocument16 pagesJaw Relation Records Guide Fixed ProsthodonticsbkprosthoNo ratings yet
- Dental Ceramics For Restoration and Metal VeneeringDocument23 pagesDental Ceramics For Restoration and Metal VeneeringMichael XuNo ratings yet
- The ProFile SystemDocument17 pagesThe ProFile SystembkprosthoNo ratings yet
- Interim Restorations PDFDocument11 pagesInterim Restorations PDFJairo RiveraNo ratings yet
- Dental Casting Alloys WatahaDocument14 pagesDental Casting Alloys WatahaClaudia MmsNo ratings yet
- Endodontic Working WidthDocument13 pagesEndodontic Working WidthbkprosthoNo ratings yet
- Classification of Removable Partial DentureDocument17 pagesClassification of Removable Partial Denturebkprostho100% (1)
- PresentationDocument16 pagesPresentationbkprosthoNo ratings yet
- Digital Dental Photography. Part 7: Extra-Oral Set-Ups: I. AhmadDocument8 pagesDigital Dental Photography. Part 7: Extra-Oral Set-Ups: I. AhmadbkprosthoNo ratings yet
- Dental OcclusionDocument10 pagesDental OcclusionFaheemuddin MuhammadNo ratings yet
- Jopr12178 PDFDocument6 pagesJopr12178 PDFbkprosthoNo ratings yet
- SJ BDJ 2009 416Document7 pagesSJ BDJ 2009 416bkprosthoNo ratings yet
- Safeguarding Children in Dentistry: 2. Do Paediatric Dentists Neglect Child Dental Neglect?Document6 pagesSafeguarding Children in Dentistry: 2. Do Paediatric Dentists Neglect Child Dental Neglect?bkprosthoNo ratings yet
- J 1532-849X 2009 00509 XDocument8 pagesJ 1532-849X 2009 00509 XbkprosthoNo ratings yet
- Digital Dental Photography. Part 8: Intra-Oral Set-Ups: I. AhmadDocument7 pagesDigital Dental Photography. Part 8: Intra-Oral Set-Ups: I. AhmadbkprosthoNo ratings yet
- Jerd 12179Document10 pagesJerd 12179bkprosthoNo ratings yet
- Palato Ram Assessment of Maxillary Comp Ete Dentures: Dauid W. Farlt, Dds,'John D. DDS, 2 Robert J. Ms3Document7 pagesPalato Ram Assessment of Maxillary Comp Ete Dentures: Dauid W. Farlt, Dds,'John D. DDS, 2 Robert J. Ms3bkprosthoNo ratings yet
- Principles of Hemodialysis: Module No: - 02 - Module TitleDocument10 pagesPrinciples of Hemodialysis: Module No: - 02 - Module TitleIan LelisNo ratings yet
- 6.3 RedoxDocument11 pages6.3 RedoxJosceline YeohNo ratings yet
- Sun & McDonough (1989) PDFDocument34 pagesSun & McDonough (1989) PDFVictor ValdiviaNo ratings yet
- Etch Rates For Micromachining Processing PDFDocument2 pagesEtch Rates For Micromachining Processing PDFJohnathanNo ratings yet
- 2nd Law Analysis of A Rankine Cycle Using The Wicks Cycle As The Ideal StandardDocument5 pages2nd Law Analysis of A Rankine Cycle Using The Wicks Cycle As The Ideal StandardCatalina Naranjo SantaellaNo ratings yet
- Chemistry Form 4 Lesson 12Document8 pagesChemistry Form 4 Lesson 12Sakinah SaadNo ratings yet
- Wave Properties of Particles ExplainedDocument19 pagesWave Properties of Particles ExplainedAmanda BoltonNo ratings yet
- Sat Vocabulary 6000 Words PDFDocument151 pagesSat Vocabulary 6000 Words PDFUman100% (1)
- Glass Ionomer Cement Properties and ApplicationsDocument67 pagesGlass Ionomer Cement Properties and ApplicationsJayalakshmi Preetha100% (1)
- Theory of PlasticityDocument10 pagesTheory of Plasticitybabu1434100% (1)
- Cold Lime Soda Softening ProcessDocument10 pagesCold Lime Soda Softening ProcessSaurabh JadhavNo ratings yet
- Introduction To Aspen Plus 2013 Tutorial VDocument77 pagesIntroduction To Aspen Plus 2013 Tutorial VsyafieqNo ratings yet
- FM Lab ManualDocument70 pagesFM Lab ManualRishi PatilNo ratings yet
- VRLA Battery White Paper Final 1Document4 pagesVRLA Battery White Paper Final 1p41005679No ratings yet
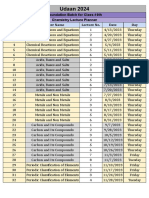
- Lecture Planner - Chemistry PDF OnlyDocument1 pageLecture Planner - Chemistry PDF OnlyJai ChandNo ratings yet
- Onqor: Product BulletinDocument2 pagesOnqor: Product BulletinAhmed ChahineNo ratings yet
- Development of A Projectile Penetration Theory. Report 1Document101 pagesDevelopment of A Projectile Penetration Theory. Report 1yararaNo ratings yet
- Reinforced Concrete Column Design QuestionsDocument4 pagesReinforced Concrete Column Design QuestionssrikanthNo ratings yet
- Pump JTN B1Document8 pagesPump JTN B1Patricia J ÁngelesNo ratings yet
- A Comparative Study of ZnO-PVP and ZnO-PEG Nanoparticles ActivityDocument8 pagesA Comparative Study of ZnO-PVP and ZnO-PEG Nanoparticles ActivityVũ Hải NamNo ratings yet
- 150 CDocument13 pages150 Crobert carbungcoNo ratings yet
- 93-1315 Deoiling ManualDocument269 pages93-1315 Deoiling ManualManash Mudoi100% (2)
- Global Warming TextsDocument3 pagesGlobal Warming TextsAnonymous NbKeZIGDVMNo ratings yet
- Non Hydrocarbon GasesDocument3 pagesNon Hydrocarbon GasesFrancelino A. X. ConceicaoNo ratings yet
- Balancing Redox Reactions by Oxidation Number Change MethodDocument4 pagesBalancing Redox Reactions by Oxidation Number Change MethodkennethmsorianoNo ratings yet
- Phase Inversion of W/O Emulsions by Adding Hydrophilic Surfactant - A Technique For Making Cosmetics ProductsDocument8 pagesPhase Inversion of W/O Emulsions by Adding Hydrophilic Surfactant - A Technique For Making Cosmetics ProductsAsshole FuckerNo ratings yet
- English Literature Syllabus BreakdownDocument35 pagesEnglish Literature Syllabus BreakdownKirti PathakNo ratings yet
- Fluid Flow PDFDocument55 pagesFluid Flow PDFHarrrison100% (1)
- GaN HEMTs - Advantages Opportunities and Challenges PDFDocument60 pagesGaN HEMTs - Advantages Opportunities and Challenges PDFghatakp2069No ratings yet
- B455Document3 pagesB455basha100% (1)
- Functional Safety from Scratch: A Practical Guide to Process Industry ApplicationsFrom EverandFunctional Safety from Scratch: A Practical Guide to Process Industry ApplicationsNo ratings yet
- Guidelines for Chemical Process Quantitative Risk AnalysisFrom EverandGuidelines for Chemical Process Quantitative Risk AnalysisRating: 5 out of 5 stars5/5 (1)
- An Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksFrom EverandAn Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksRating: 5 out of 5 stars5/5 (1)
- Guidelines for the Management of Change for Process SafetyFrom EverandGuidelines for the Management of Change for Process SafetyNo ratings yet
- Piping and Pipeline Calculations Manual: Construction, Design Fabrication and ExaminationFrom EverandPiping and Pipeline Calculations Manual: Construction, Design Fabrication and ExaminationRating: 4 out of 5 stars4/5 (18)
- Nuclear Energy in the 21st Century: World Nuclear University PressFrom EverandNuclear Energy in the 21st Century: World Nuclear University PressRating: 4.5 out of 5 stars4.5/5 (3)
- Trevor Kletz Compendium: His Process Safety Wisdom Updated for a New GenerationFrom EverandTrevor Kletz Compendium: His Process Safety Wisdom Updated for a New GenerationNo ratings yet
- Guidelines for Siting and Layout of FacilitiesFrom EverandGuidelines for Siting and Layout of FacilitiesNo ratings yet
- Process Engineering for a Small Planet: How to Reuse, Re-Purpose, and Retrofit Existing Process EquipmentFrom EverandProcess Engineering for a Small Planet: How to Reuse, Re-Purpose, and Retrofit Existing Process EquipmentNo ratings yet
- Well Control for Completions and InterventionsFrom EverandWell Control for Completions and InterventionsRating: 4 out of 5 stars4/5 (10)
- Guidelines for Vapor Cloud Explosion, Pressure Vessel Burst, BLEVE, and Flash Fire HazardsFrom EverandGuidelines for Vapor Cloud Explosion, Pressure Vessel Burst, BLEVE, and Flash Fire HazardsNo ratings yet
- Guidelines for Enabling Conditions and Conditional Modifiers in Layer of Protection AnalysisFrom EverandGuidelines for Enabling Conditions and Conditional Modifiers in Layer of Protection AnalysisNo ratings yet
- An Applied Guide to Water and Effluent Treatment Plant DesignFrom EverandAn Applied Guide to Water and Effluent Treatment Plant DesignRating: 5 out of 5 stars5/5 (4)
- Robotics: Designing the Mechanisms for Automated MachineryFrom EverandRobotics: Designing the Mechanisms for Automated MachineryRating: 4.5 out of 5 stars4.5/5 (8)
- Guidelines for Developing Quantitative Safety Risk CriteriaFrom EverandGuidelines for Developing Quantitative Safety Risk CriteriaNo ratings yet
- Chemical Process Safety: Learning from Case HistoriesFrom EverandChemical Process Safety: Learning from Case HistoriesRating: 4 out of 5 stars4/5 (14)
- Guidelines for Engineering Design for Process SafetyFrom EverandGuidelines for Engineering Design for Process SafetyNo ratings yet
- Perfume Engineering: Design, Performance and ClassificationFrom EverandPerfume Engineering: Design, Performance and ClassificationRating: 4 out of 5 stars4/5 (5)
- Temperature-Responsive Polymers: Chemistry, Properties, and ApplicationsFrom EverandTemperature-Responsive Polymers: Chemistry, Properties, and ApplicationsNo ratings yet
- The HAZOP Leader's Handbook: How to Plan and Conduct Successful HAZOP StudiesFrom EverandThe HAZOP Leader's Handbook: How to Plan and Conduct Successful HAZOP StudiesNo ratings yet
- Bow Ties in Risk Management: A Concept Book for Process SafetyFrom EverandBow Ties in Risk Management: A Concept Book for Process SafetyNo ratings yet