You might also like
- SAS overviewDocument4 pagesSAS overviewEdosa Joshua Aronmwan86% (21)
- Example Assignment 7003Document14 pagesExample Assignment 7003Javeriah Arif75% (4)
- Comments On COA-PETDocument1 pageComments On COA-PETAddy GuinalNo ratings yet
- SFM Case 4 Strategic ValuationDocument3 pagesSFM Case 4 Strategic ValuationPatrick RomeroNo ratings yet
- Disbursement Voucher: DPWH-Sorsogon 1st DEODocument24 pagesDisbursement Voucher: DPWH-Sorsogon 1st DEOTIMMY BOY100% (1)
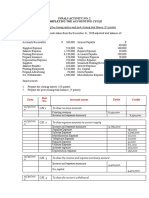
- Nerissa Mae L. Santos Activity On Completing The Accounting Cycle 1Document3 pagesNerissa Mae L. Santos Activity On Completing The Accounting Cycle 1Mica Mae Correa100% (1)
- GAM Forms 2016Document27 pagesGAM Forms 2016Grace Dela CruzNo ratings yet
- Travel OrderDocument4 pagesTravel OrderAldrin NolascoNo ratings yet
- No.: - Date: - Agency FundDocument12 pagesNo.: - Date: - Agency Fundlegal.darposaranganiNo ratings yet
- A. B. Certified: Certified: Allotment Available and ObligatedDocument3 pagesA. B. Certified: Certified: Allotment Available and ObligatedMatias WinnerNo ratings yet
- Budget Utilization Request StatusDocument11 pagesBudget Utilization Request Statusjef repuldaNo ratings yet
- Obligation Request and StatusDocument12 pagesObligation Request and Statusmichael ricafortNo ratings yet
- No.: - Date: - Agency FundDocument11 pagesNo.: - Date: - Agency Fundlegal.darposaranganiNo ratings yet
- Travel Antipuesto 0621 252022Document21 pagesTravel Antipuesto 0621 252022Gwendolyn Lalamonan AnganaNo ratings yet
- DISBURSEMENT VOUCHER (JC) - AugustDocument2 pagesDISBURSEMENT VOUCHER (JC) - Augusthekeho3180No ratings yet
- Obligation Request and Status: Dilg Car Entity Name Dilg Car Cos Personnel-Contact TracersDocument3 pagesObligation Request and Status: Dilg Car Entity Name Dilg Car Cos Personnel-Contact TracersClaudine PuyaoNo ratings yet
- Processing and Payment of Claims Checklist: Travel Expenses Local TravelDocument6 pagesProcessing and Payment of Claims Checklist: Travel Expenses Local TravelLorna De CastroNo ratings yet
- Budget Utilization Request and Status: Nenita L.MarcosDocument2 pagesBudget Utilization Request and Status: Nenita L.MarcosMemphis RainsNo ratings yet
- Summary List of Supporting DocumentsDocument11 pagesSummary List of Supporting DocumentsJeshree jean RomeroNo ratings yet
- Disbursement VoucherDocument1 pageDisbursement VoucherDebbie Ann ArdenioNo ratings yet
- Liam BolecheDocument5 pagesLiam BolechemayrubienythNo ratings yet
- Dss 1Document1 pageDss 1Jessica JaroNo ratings yet
- Obligation Request and Status: Appendix 11Document2 pagesObligation Request and Status: Appendix 11Rogie ApoloNo ratings yet
- Supplier 1 Supplier 2 Supplier 3 Surigao City Under Advertisement and Canvass Number 001-003 Opened atDocument7 pagesSupplier 1 Supplier 2 Supplier 3 Surigao City Under Advertisement and Canvass Number 001-003 Opened atAisa Lagutin TadulanNo ratings yet
- Appendix 14 - BURSDocument1 pageAppendix 14 - BURSMark Joseph BajaNo ratings yet
- Obligation Request and Status Budget Utilization Request and StatusDocument2 pagesObligation Request and Status Budget Utilization Request and StatusKatrina SedilloNo ratings yet
- Obligation Request and Status: Appendix 11Document45 pagesObligation Request and Status: Appendix 11Kevin Verdan CambaNo ratings yet
- Bustonera Chito Noel D. July2022 GADocument3 pagesBustonera Chito Noel D. July2022 GAJohn Carlo D. EngayNo ratings yet
- SarahDocument4 pagesSarahmayrubienythNo ratings yet
- Appendix 32 DVDocument1 pageAppendix 32 DVkagami aNo ratings yet
- FURS-1Document1 pageFURS-1YHONG SILVANONo ratings yet
- Template AnnexesDocument73 pagesTemplate AnnexesGaming With LanzNo ratings yet
- Obligation Status and Check ReportDocument2 pagesObligation Status and Check ReportjosephNo ratings yet
- VoucherDocument4 pagesVoucherBplo CaloocanNo ratings yet
- Cash Advance UPDocument18 pagesCash Advance UPJohannes Gregorii LagueNo ratings yet
- Obligation Request and Status: Appendix 11Document2 pagesObligation Request and Status: Appendix 11Cj NightsirkNo ratings yet
- Forms NewDocument99 pagesForms NewvernaNo ratings yet
- Agriculture Appendix 32 FundsDocument1 pageAgriculture Appendix 32 FundsKim MonteronaNo ratings yet
- Sir PioDocument8 pagesSir PioREGIONAL DIRECTOR SOUTHERN TAGALOG0% (1)
- Disbursement Voucher - DepEdDocument1 pageDisbursement Voucher - DepEdJ LNo ratings yet
- Itenerary of Travel-Casanova SPPFDocument4 pagesItenerary of Travel-Casanova SPPFCj NightsirkNo ratings yet
- Disbursement Voucher DV 1Document2 pagesDisbursement Voucher DV 1JudyAnIntongQuiroyNo ratings yet
- ORS 2021 (AutoRecovered)Document23 pagesORS 2021 (AutoRecovered)Theresa Faye De GuzmanNo ratings yet
- To Payment of Electricity Expenses For The Period of - As Per Billing Statement Hereto AttachedDocument6 pagesTo Payment of Electricity Expenses For The Period of - As Per Billing Statement Hereto AttachedShiela E. EladNo ratings yet
- Disbursement Voucher: Diannee Antoniettee L. EnriquezDocument1 pageDisbursement Voucher: Diannee Antoniettee L. EnriquezShyne peraltaNo ratings yet
- Gagers Travel VoucherDocument1 pageGagers Travel VoucherNeølie Abello LatúrnasNo ratings yet
- Reimbursement Travel Expenses MasbateDocument4 pagesReimbursement Travel Expenses MasbateJovelyn SeseNo ratings yet
- Travelling Electricity Office Supplies Other Supplies Fidelity Bond Other Mooe Bank ChargesDocument17 pagesTravelling Electricity Office Supplies Other Supplies Fidelity Bond Other Mooe Bank ChargesElaine LabaoNo ratings yet
- Appendix 32 DVDocument1 pageAppendix 32 DVRhinelle PescadorNo ratings yet
- Mooe School Forms 2020Document40 pagesMooe School Forms 2020Bat RicNo ratings yet
- New Mooe FormsDocument14 pagesNew Mooe FormsMark Lorence CezarNo ratings yet
- Appendix 11 ORSDocument4 pagesAppendix 11 ORSgennadacaweNo ratings yet
- BIIS Blank DV and 2307Document3 pagesBIIS Blank DV and 2307spayumo821No ratings yet
- NEW FORMAT-voucherDocument20 pagesNEW FORMAT-voucherRalph Sison ReyesNo ratings yet
- Disbursement VoucherDocument1 pageDisbursement VoucherGeorgina Intia100% (1)
- Municipality of Guipos: Republic of The Philippines Province of Zamboanga de SurDocument21 pagesMunicipality of Guipos: Republic of The Philippines Province of Zamboanga de SurMelvinson Loui Polenzo SarcaugaNo ratings yet
- DV TemplateDocument4 pagesDV TemplateLeah TubangNo ratings yet
- Report of Checks Issued (RCI) For SchoolsDocument4 pagesReport of Checks Issued (RCI) For Schoolsamender22No ratings yet
- Disbursement Voucher DV 1Document2 pagesDisbursement Voucher DV 1Mark HernandezNo ratings yet
- Funds DisbursedDocument6 pagesFunds DisbursedShiela E. EladNo ratings yet
- Obligation Request (ObR)Document2 pagesObligation Request (ObR)Lester CuanicoNo ratings yet
- Ob. Req. New Form (2016)Document2 pagesOb. Req. New Form (2016)First NameNo ratings yet
- Vouchers SampleDocument1 pageVouchers SampleLex AmarieNo ratings yet
- ORS DV-d.o.Document2 pagesORS DV-d.o.Jessica CrisostomoNo ratings yet
- BIR memorandum on tax investigationDocument2 pagesBIR memorandum on tax investigationAddy GuinalNo ratings yet
- EOPTDocument6 pagesEOPTAddy GuinalNo ratings yet
- JAN0GR01R047414Document2 pagesJAN0GR01R047414John Nelson A PiconesNo ratings yet
- RR No. 11-2018 amends tax withholding provisionsDocument38 pagesRR No. 11-2018 amends tax withholding provisionsMo MuNo ratings yet
- Labor Seat PlanDocument2 pagesLabor Seat PlanAddy GuinalNo ratings yet
- COA orders suspension of salaries for delay in financial report submissionDocument1 pageCOA orders suspension of salaries for delay in financial report submissionAddy GuinalNo ratings yet
- Provisions on Accretion and Capacity to InheritDocument11 pagesProvisions on Accretion and Capacity to InheritAddy GuinalNo ratings yet
- Provisions on Accretion and Capacity to InheritDocument11 pagesProvisions on Accretion and Capacity to InheritAddy GuinalNo ratings yet
- Concepts OwnershipDocument24 pagesConcepts OwnershipAddy GuinalNo ratings yet
- COA Cirular 85-55-ADocument19 pagesCOA Cirular 85-55-AJesus Carlo Adalla QuirapNo ratings yet
- 1 NREL ReviewerDocument16 pages1 NREL Reviewer'Joshua Crisostomo'No ratings yet
- EXPEDITING ENVIRONMENTAL PROCEEDINGSDocument1 pageEXPEDITING ENVIRONMENTAL PROCEEDINGSAddy GuinalNo ratings yet
- Roman Catholic Vs CADocument2 pagesRoman Catholic Vs CAAddy GuinalNo ratings yet
- AuthorizationDocument1 pageAuthorizationAddy GuinalNo ratings yet
- Admin Digest - Kilusang Bayan V DominguezDocument2 pagesAdmin Digest - Kilusang Bayan V DominguezHoven Macasinag100% (1)
- Toyota Vs de GuzmanDocument1 pageToyota Vs de GuzmanAddy GuinalNo ratings yet
- Civ Pro BeiDocument4 pagesCiv Pro BeiAddy GuinalNo ratings yet
- Airline Pilots Vs CIRDocument3 pagesAirline Pilots Vs CIRAddy GuinalNo ratings yet
- Reviewer 2018Document3 pagesReviewer 2018Addy GuinalNo ratings yet
- Association de Agricultores Vs TalisayDocument74 pagesAssociation de Agricultores Vs TalisayAddy GuinalNo ratings yet
- Airline Pilots Vs CIRDocument12 pagesAirline Pilots Vs CIRAddy GuinalNo ratings yet
- 1Document1 page1Addy GuinalNo ratings yet
- Aapsi ML 2014 - 3.8.2016Document45 pagesAapsi ML 2014 - 3.8.2016Addy GuinalNo ratings yet
- PCI Leasing Vs GiraffeDocument1 pagePCI Leasing Vs GiraffeAddy Guinal100% (3)
- Purple Notes Insurance 2010Document40 pagesPurple Notes Insurance 2010Addy GuinalNo ratings yet
- Request Letter2Document1 pageRequest Letter2Addy GuinalNo ratings yet
- ALU Vs CallejaDocument2 pagesALU Vs CallejaAddy GuinalNo ratings yet
- Crim Pro DigestDocument3 pagesCrim Pro DigestAddy GuinalNo ratings yet
- Insurance Dispute Over Burned PropertyDocument12 pagesInsurance Dispute Over Burned PropertyAddy GuinalNo ratings yet
- Assignment MIS320.1 SUBMITTED TO: Kabid MD Surid, Department of Management Date of Submission: 06.01.2021Document7 pagesAssignment MIS320.1 SUBMITTED TO: Kabid MD Surid, Department of Management Date of Submission: 06.01.2021Sk. Shahriar RahmanNo ratings yet
- Gspbookstore - LOCAL ACAD As of 03.01.2021Document9 pagesGspbookstore - LOCAL ACAD As of 03.01.2021Russ AndresNo ratings yet
- BP - AkuntansiDocument73 pagesBP - AkuntansiUlin HsbNo ratings yet
- PAPS-1000Ph Revised FinalDocument11 pagesPAPS-1000Ph Revised FinalNigelT.LeeNo ratings yet
- 8m Work CertDocument1 page8m Work CertAdrian DoruNo ratings yet
- 07 JUNE QuestionDocument11 pages07 JUNE Questionkhengmai67% (3)
- SU14 Deloitte Cover Letter ReviewDocument1 pageSU14 Deloitte Cover Letter ReviewĐinh Như Thủy HằngNo ratings yet
- 2022 - FMGT2152 Course OutlineDocument3 pages2022 - FMGT2152 Course OutlineKCNo ratings yet
- SyllabusDocument8 pagesSyllabusAntônio DuarteNo ratings yet
- Full Download Financial Accounting Theory and Analysis Text and Cases 10th Edition Schroeder Test BankDocument35 pagesFull Download Financial Accounting Theory and Analysis Text and Cases 10th Edition Schroeder Test BankjosephkvqhperezNo ratings yet
- Ahlan Nur Salim - Tugas 3Document4 pagesAhlan Nur Salim - Tugas 3Moe ChannelNo ratings yet
- Sap Fi End User Practice Work: AR AP Asset AccountingDocument19 pagesSap Fi End User Practice Work: AR AP Asset AccountingHany RefaatNo ratings yet
- UAS-AKL 1 - IntlDocument2 pagesUAS-AKL 1 - IntlSweda ArifahNo ratings yet
- Fiscal Managemant Day 1Document90 pagesFiscal Managemant Day 1C.j. TenorioNo ratings yet
- Sec Form Exa-001Document3 pagesSec Form Exa-001Rheneir MoraNo ratings yet
- LaporanKeuanganWIKA30September2018Document164 pagesLaporanKeuanganWIKA30September2018arrizal firdausNo ratings yet
- AIS Chapter 1Document46 pagesAIS Chapter 1Ma. Elene MagdaraogNo ratings yet
- FICO STD ReportsDocument12 pagesFICO STD Reportsshekar8876100% (1)
- CA Program Timetable Yearly Term 1 2023 - Term 4 2024Document3 pagesCA Program Timetable Yearly Term 1 2023 - Term 4 2024NXTKILLERX GamingNo ratings yet
- AccountingDocument8 pagesAccountingYaredNo ratings yet
- CH 11Document55 pagesCH 11Bhavin purohitNo ratings yet
- CPA Auditing Practice QuestionsDocument4 pagesCPA Auditing Practice Questionsswit_kamote100% (1)
- Cash Book: ModuleDocument21 pagesCash Book: ModuleTushar SainiNo ratings yet
- LMPC Job OpeningsDocument33 pagesLMPC Job OpeningsRea Ann Autor LiraNo ratings yet
- Lecture Week 3Document54 pagesLecture Week 3soliman salmanNo ratings yet
- University of Kerala: Regulation, Scheme and SyllabusDocument98 pagesUniversity of Kerala: Regulation, Scheme and SyllabusyogeshNo ratings yet