You might also like
- Animal Policy Final 012717 PDFDocument13 pagesAnimal Policy Final 012717 PDFcommanderkeenNo ratings yet
- Service and Assistance Animal PolicyDocument9 pagesService and Assistance Animal PolicycommanderkeenNo ratings yet
- ACFormDocument5 pagesACFormcommanderkeen100% (1)
- Service, Assistance, and Other Animals at Northwestern Policy StatementDocument13 pagesService, Assistance, and Other Animals at Northwestern Policy StatementcommanderkeenNo ratings yet
- Service-Assistance Animal Policy in University HousingDocument6 pagesService-Assistance Animal Policy in University HousingcommanderkeenNo ratings yet
- 036 CDocument12 pages036 CcommanderkeenNo ratings yet
- Goat Medications 2015Document3 pagesGoat Medications 2015commanderkeenNo ratings yet
- Columbia University Service and Assistance Animal PolicyDocument10 pagesColumbia University Service and Assistance Animal PolicycommanderkeenNo ratings yet
- Service-Assistance Animal Policy in University Housing PDFDocument6 pagesService-Assistance Animal Policy in University Housing PDFcommanderkeenNo ratings yet
- Physical Activity and Exercise Recent Advances and Current ChallengesDocument11 pagesPhysical Activity and Exercise Recent Advances and Current ChallengescommanderkeenNo ratings yet
- Assistance Animal Policy and AgreementDocument5 pagesAssistance Animal Policy and AgreementcommanderkeenNo ratings yet
- Animal RequestDocument5 pagesAnimal RequestcommanderkeenNo ratings yet
- Edrv0521 PDFDocument27 pagesEdrv0521 PDFcommanderkeenNo ratings yet
- Analyzing Political CartoonsDocument1 pageAnalyzing Political CartoonscommanderkeenNo ratings yet
- Ddsig Fact Sheet Exercise and Post Polio Syndrome PDFDocument3 pagesDdsig Fact Sheet Exercise and Post Polio Syndrome PDFcommanderkeenNo ratings yet
- 147 12 1175 PDFDocument2 pages147 12 1175 PDFcommanderkeenNo ratings yet
- Analyzing Political Cartoons PDFDocument1 pageAnalyzing Political Cartoons PDFcommanderkeenNo ratings yet
- Special Report: Vitamins and MineralsDocument8 pagesSpecial Report: Vitamins and MineralscommanderkeenNo ratings yet
- Eds 21 ManualDocument9 pagesEds 21 ManualcommanderkeenNo ratings yet
- Vitamin D Sip43 June14 PDFDocument11 pagesVitamin D Sip43 June14 PDFcommanderkeenNo ratings yet
- Special Report: Vitamins and MineralsDocument8 pagesSpecial Report: Vitamins and MineralscommanderkeenNo ratings yet
- Foods With Vitamin K PDFDocument2 pagesFoods With Vitamin K PDFcommanderkeenNo ratings yet
- Vitamin D Brochure FINALDocument3 pagesVitamin D Brochure FINALcommanderkeenNo ratings yet
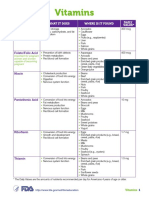
- Vitamin and Mineral Chart PDFDocument5 pagesVitamin and Mineral Chart PDFcommanderkeenNo ratings yet
- ARGFocus 201008 VitaminsDAK WebDocument16 pagesARGFocus 201008 VitaminsDAK WebcommanderkeenNo ratings yet
- Edrv 0521Document27 pagesEdrv 0521commanderkeenNo ratings yet
- Efsa - Tolerable Upper Intake LevelsDocument482 pagesEfsa - Tolerable Upper Intake LevelsdrantistNo ratings yet
- Vitamin A Deficiency: Health, Survival and Vision: by Alfred Sommer and Keith P. WestDocument2 pagesVitamin A Deficiency: Health, Survival and Vision: by Alfred Sommer and Keith P. WestcommanderkeenNo ratings yet
- FINAL VERSION National Guidelines VAS3 PDFDocument2 pagesFINAL VERSION National Guidelines VAS3 PDFcommanderkeenNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 1 Introduction To Biochem, Energy, and MetabolismDocument4 pages1 Introduction To Biochem, Energy, and MetabolismVILLAMOR, CAMILA D.No ratings yet
- Protein Nutrition (David Bender)Document68 pagesProtein Nutrition (David Bender)Anonymous 8h8Rw6YmAnNo ratings yet
- Q1.The Diagram Shows A Mitochondrion.: Feversham CollegeDocument56 pagesQ1.The Diagram Shows A Mitochondrion.: Feversham CollegeZaksd100% (1)
- Importance of Carbohydrate Metabolism in Human Body: Fig.1 - Glucose StructureDocument4 pagesImportance of Carbohydrate Metabolism in Human Body: Fig.1 - Glucose StructureRimsha EramNo ratings yet
- 06 9700 42 2013 62592.inddDocument2 pages06 9700 42 2013 62592.inddRaphael JosephNo ratings yet
- Frac Moa Poster FungicidasDocument1 pageFrac Moa Poster Fungicidaskelvin horna guiopNo ratings yet
- BiochemEngg ReportDocument14 pagesBiochemEngg ReportJenny LlanesNo ratings yet
- 2-Cell EnergyDocument4 pages2-Cell Energyapi-238421605No ratings yet
- Lecture 1 - Introduction To Secondary MetabolitesDocument36 pagesLecture 1 - Introduction To Secondary MetabolitesAlec LiuNo ratings yet
- ELS Q2 M3 Introduction To Life ScienceDocument20 pagesELS Q2 M3 Introduction To Life ScienceKath Tan Alcantara86% (7)
- Bacterial Contaminants and Their Effects On Alcohol ProductionDocument18 pagesBacterial Contaminants and Their Effects On Alcohol ProductionJesus LucesNo ratings yet
- Catabolism of Proteins and Amino Acid NitrogenDocument6 pagesCatabolism of Proteins and Amino Acid Nitrogenyel5buscatoNo ratings yet
- Lesson 7.1 Inborn Errors of MetabolismDocument119 pagesLesson 7.1 Inborn Errors of Metabolismmisaki06100% (2)
- Glycogen MetabolismDocument23 pagesGlycogen Metabolismessa100% (1)
- OSTEOMALACIADocument10 pagesOSTEOMALACIAaeruginoNo ratings yet
- Glycogen Synthesis and DegradationDocument2 pagesGlycogen Synthesis and DegradationYashimera Laid MaapeNo ratings yet
- Cyclic PhotophosphorylationDocument10 pagesCyclic PhotophosphorylationJenard Atos33% (3)
- B.SC - Nursing 1st Year PDFDocument9 pagesB.SC - Nursing 1st Year PDFSunita RaniNo ratings yet
- Lecture 9 - Carbohydrates StructureDocument36 pagesLecture 9 - Carbohydrates StructureHabib Abou ShahineNo ratings yet
- University of Gondar Biology Department IntroductionDocument238 pagesUniversity of Gondar Biology Department IntroductionAlemayehu MelkamuuNo ratings yet
- Metabolic Liver DiseaseDocument23 pagesMetabolic Liver DiseaseHal ChenNo ratings yet
- Hormones and Nutrient PartitioningDocument36 pagesHormones and Nutrient Partitioningbwade2_916499061No ratings yet
- Semi-Detailed Lesson PlanDocument3 pagesSemi-Detailed Lesson Planjoselyn bergonia100% (1)
- Carbohydrate Metabolism: Blood Haemoglobin and Respiration: - Archit SaraogiDocument6 pagesCarbohydrate Metabolism: Blood Haemoglobin and Respiration: - Archit SaraogiChictoran RukmaniNo ratings yet
- CC1 Intro To Lipids 2016Document60 pagesCC1 Intro To Lipids 2016Patrisha BuanNo ratings yet
- Boards SyllabusDocument14 pagesBoards Syllabus2012No ratings yet
- Nutrient Utilization in HumansDocument5 pagesNutrient Utilization in Humansxiomara alarcon sierraNo ratings yet
- Unit 1: Scope of Clinical ChemistryDocument79 pagesUnit 1: Scope of Clinical ChemistryMegumi TadokoroNo ratings yet
- 9700 BIOLOGY: MARK SCHEME For The May/June 2012 Question Paper For The Guidance of TeachersDocument14 pages9700 BIOLOGY: MARK SCHEME For The May/June 2012 Question Paper For The Guidance of Teacherslianghoo94No ratings yet
- SHS STEM Bio1 Q2 Week 3 Module 5 - Aerobic Vs Anaerobic RespirationDocument19 pagesSHS STEM Bio1 Q2 Week 3 Module 5 - Aerobic Vs Anaerobic RespirationRomel Bayaban100% (2)