You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- No Fry Fried RiceDocument1 pageNo Fry Fried RiceRoisinNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Watermelon and Feta SaladDocument1 pageWatermelon and Feta SaladRoisinNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Curried Potato PastiesDocument2 pagesCurried Potato PastiesRoisinNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Belfast PlanoDocument2 pagesBelfast PlanoCaro DiazNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
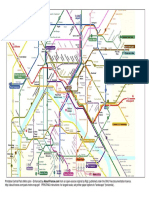
- Printable Paris Metro MapDocument2 pagesPrintable Paris Metro MapRoisinNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Cardiovascular Circuit Training WorkoutDocument1 pageCardiovascular Circuit Training WorkoutRoisinNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Roasted Spring Vegetables - Bless This MessDocument2 pagesRoasted Spring Vegetables - Bless This MessRoisinNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Versailles Palace: ParisDocument2 pagesVersailles Palace: ParisRoisinNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Homemade Chicken Nuggets: IngredientsDocument2 pagesHomemade Chicken Nuggets: IngredientsRoisinNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Mexican Restaurant-Style Cauliflower RiceDocument2 pagesMexican Restaurant-Style Cauliflower RiceRoisinNo ratings yet
- Campusmap PDFDocument2 pagesCampusmap PDFDenis DalliNo ratings yet
- Banana Muffins: IngredientsDocument1 pageBanana Muffins: IngredientsRoisinNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Conditions of Assistance for Part Time Study & CPDDocument2 pagesConditions of Assistance for Part Time Study & CPDRoisinNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Exercise count-up workout trackerDocument2 pagesExercise count-up workout trackerRoisinNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- FitnessAssessment 2015 16 PDFDocument16 pagesFitnessAssessment 2015 16 PDFlaxave8817No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Leaflet Physical Activity Recommendations PDFDocument2 pagesLeaflet Physical Activity Recommendations PDFRoisinNo ratings yet
- Delayed Onset Muscle Soreness (Doms)Document2 pagesDelayed Onset Muscle Soreness (Doms)steffiecruz06No ratings yet
- Trust SoundtrackDocument2 pagesTrust SoundtrackRoisinNo ratings yet
- Physical Activity and Common Mental DisordersDocument9 pagesPhysical Activity and Common Mental DisordersRoisinNo ratings yet
- Folic AcidDocument2 pagesFolic AcidRoisinNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Trans FatsDocument2 pagesTrans FatsRoisinNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- n55 Australian Dietary Guidelines 130530 PDFDocument226 pagesn55 Australian Dietary Guidelines 130530 PDFtech1322No ratings yet
- Files 10624pfibrosarcomaDocument4 pagesFiles 10624pfibrosarcomaLily NGNo ratings yet
- Vegetarian Food FactsDocument2 pagesVegetarian Food FactsRoisinNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- A Guide For Exercising During and After Treatment For Cancer PDFDocument20 pagesA Guide For Exercising During and After Treatment For Cancer PDFRoisinNo ratings yet
- Health & Fitness Journal: of CanadaDocument13 pagesHealth & Fitness Journal: of CanadaRoisinNo ratings yet
- PregnancyDocument2 pagesPregnancyRoisinNo ratings yet
- Starting An Exercise Program: Health and Medical Questionnaire Fitness Assessment Informed ConsentDocument2 pagesStarting An Exercise Program: Health and Medical Questionnaire Fitness Assessment Informed ConsentRoisinNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- How To Work With Health Care Providers: A Systematic ApproachDocument8 pagesHow To Work With Health Care Providers: A Systematic ApproachRoisinNo ratings yet
- CANAL (T) Canal Soth FloridaDocument115 pagesCANAL (T) Canal Soth FloridaMIKHA2014No ratings yet
- Laser Surface Treatment ProcessesDocument63 pagesLaser Surface Treatment ProcessesDIPAK VINAYAK SHIRBHATENo ratings yet
- LKC CS Assignment2Document18 pagesLKC CS Assignment2Jackie LeongNo ratings yet
- PDFViewer - JSP 3Document46 pagesPDFViewer - JSP 3Kartik ChaudharyNo ratings yet
- Library Dissertation in Community DentistryDocument9 pagesLibrary Dissertation in Community DentistryPayForPaperCanada100% (1)
- The Apu Trilogy - Robin Wood PDFDocument48 pagesThe Apu Trilogy - Robin Wood PDFSamkush100% (1)
- Sri Radhakrishna SwamijiDocument43 pagesSri Radhakrishna SwamijiNarayana IyengarNo ratings yet
- Application of Fertility Capability Classification System in Rice Growing Soils of Damodar Command Area, West Bengal, IndiaDocument9 pagesApplication of Fertility Capability Classification System in Rice Growing Soils of Damodar Command Area, West Bengal, IndiaDr. Ranjan BeraNo ratings yet
- Space DynamicsDocument37 pagesSpace Dynamicspurushottam KashyapNo ratings yet
- Monster of The Week Tome of Mysteries PlaybooksDocument10 pagesMonster of The Week Tome of Mysteries PlaybooksHyperLanceite XNo ratings yet
- Stability Calculation of Embedded Bolts For Drop Arm Arrangement For ACC Location Inside TunnelDocument7 pagesStability Calculation of Embedded Bolts For Drop Arm Arrangement For ACC Location Inside TunnelSamwailNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Caterpillar Ep15krtDocument37 pagesCaterpillar Ep15krtIvan MajikNo ratings yet
- Fundermax Exterior Technic 2011gb WebDocument88 pagesFundermax Exterior Technic 2011gb WebarchpavlovicNo ratings yet
- Troubleshooting Hydraulic Circuits: Fluid PowerDocument32 pagesTroubleshooting Hydraulic Circuits: Fluid PowerMi LuanaNo ratings yet
- Ricoh 4055 PDFDocument1,280 pagesRicoh 4055 PDFPham Nguyen Hoang Minh100% (1)
- MS For Brick WorkDocument7 pagesMS For Brick WorkSumit OmarNo ratings yet
- Railway Airport Docks and HarbourDocument21 pagesRailway Airport Docks and HarbourvalarmathibalanNo ratings yet
- Swami Rama's demonstration of voluntary control over autonomic functionsDocument17 pagesSwami Rama's demonstration of voluntary control over autonomic functionsyunjana100% (1)
- SRS Design Guidelines PDFDocument46 pagesSRS Design Guidelines PDFLia FernandaNo ratings yet
- Chemistry of FormazanDocument36 pagesChemistry of FormazanEsteban ArayaNo ratings yet
- Air Arms S400 EXPDocument3 pagesAir Arms S400 EXPapi-3695814No ratings yet
- Material and Energy Balance: PN Husna Binti ZulkiflyDocument108 pagesMaterial and Energy Balance: PN Husna Binti ZulkiflyFiras 01No ratings yet
- Thermal BurnsDocument50 pagesThermal BurnsPooya WindyNo ratings yet
- House Designs, QHC, 1950Document50 pagesHouse Designs, QHC, 1950House Histories100% (8)
- O2 Orthodontic Lab Catalog PDFDocument20 pagesO2 Orthodontic Lab Catalog PDFplayer osamaNo ratings yet
- Front Wheel Steering System With Movable Hedlights Ijariie5360Document6 pagesFront Wheel Steering System With Movable Hedlights Ijariie5360Ifra KhanNo ratings yet
- Canon imageFORMULA DR-X10CDocument208 pagesCanon imageFORMULA DR-X10CYury KobzarNo ratings yet
- Gautam Samhita CHP 1 CHP 2 CHP 3 ColorDocument22 pagesGautam Samhita CHP 1 CHP 2 CHP 3 ColorSaptarishisAstrology100% (1)
- ADDRESSABLE 51.HI 60854 G Contoller GuideDocument76 pagesADDRESSABLE 51.HI 60854 G Contoller Guidemohinfo88No ratings yet
- Chakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.From EverandChakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.Rating: 4 out of 5 stars4/5 (2)
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingFrom EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingRating: 4.5 out of 5 stars4.5/5 (66)
- Hero Maker: 12 Weeks to Superhero Fit: A Hollywood Trainer's REAL Guide to Getting the Body You've Always WantedFrom EverandHero Maker: 12 Weeks to Superhero Fit: A Hollywood Trainer's REAL Guide to Getting the Body You've Always WantedRating: 4 out of 5 stars4/5 (1)
- The Yogi Code: Seven Universal Laws of Infinite SuccessFrom EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessRating: 4.5 out of 5 stars4.5/5 (104)
- Calisthenics: Guide for Bodyweight Exercise, Build your Dream Body in 30 MinutesFrom EverandCalisthenics: Guide for Bodyweight Exercise, Build your Dream Body in 30 MinutesRating: 3 out of 5 stars3/5 (5)
- Relentless: From Good to Great to UnstoppableFrom EverandRelentless: From Good to Great to UnstoppableRating: 5 out of 5 stars5/5 (780)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindFrom EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindRating: 4.5 out of 5 stars4.5/5 (1)